|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
UNDERSTANDING THE MODERN PROGRESSION OF FACTS & MYTHS ABOUT "SEXUALITY" By Pierre J. Tremblay in Collaboration with Richard Ramsay Faculty of Social Work, University of Calgary. Abstract
|






 These
definitions, categories, and related labels, however, were not always so, as
asserted by Michel Foucault (
These
definitions, categories, and related labels, however, were not always so, as
asserted by Michel Foucault (Male Sexual Intimacy: From Common to a Rarity?
 In
1960, I was 10-years-old and growing up in a working class environment where
male homosexual activity was the rule,
not the exception. Its predominant manifestation was "sex with equality,"
thus including mutual masturbation and oral sex,
but not anal sex
(Bagley, 1997, p. 183).
The latter was not even thought about, except for eventually
learning that passive anal sex was an activity engaged in by apparently degraded
males who thought themselves to be like women, or were labeled as such because
they were accepting the status of being anally penetrated. As for ourselves
living in a world where effeminate males did not exist, our sexual activities
with other males generally reflected our social relationships: most sex with
one's best friend, and lesser sex with lesser friends. We also had girlfriends
and knew what was to be done sexually with them as it was so well understood via
having learned the word "fuck" and its clear meaning. This explains why even the
thought of "fucking" one's best friend was precluded: the activity or related
desires was in violation of our equality based male bonding friendships. Sexual
activity was also only a small part of our daily activities, and it was not an
everyday activity although, at times, it was enjoyed more than once a day.
In
1960, I was 10-years-old and growing up in a working class environment where
male homosexual activity was the rule,
not the exception. Its predominant manifestation was "sex with equality,"
thus including mutual masturbation and oral sex,
but not anal sex
(Bagley, 1997, p. 183).
The latter was not even thought about, except for eventually
learning that passive anal sex was an activity engaged in by apparently degraded
males who thought themselves to be like women, or were labeled as such because
they were accepting the status of being anally penetrated. As for ourselves
living in a world where effeminate males did not exist, our sexual activities
with other males generally reflected our social relationships: most sex with
one's best friend, and lesser sex with lesser friends. We also had girlfriends
and knew what was to be done sexually with them as it was so well understood via
having learned the word "fuck" and its clear meaning. This explains why even the
thought of "fucking" one's best friend was precluded: the activity or related
desires was in violation of our equality based male bonding friendships. Sexual
activity was also only a small part of our daily activities, and it was not an
everyday activity although, at times, it was enjoyed more than once a day.
As a young adult, I ventured into learning more about male homosexuality and encountered the Kinsey et al. (1948) study which contained data not at odds with my experiences (Note 3), nor with the similar experiences of my youngest brother who grew up in the same neighborhood. Although he did not engage in homosexual activity, when asked what our neighborhood was like in the 1970s, he explained the male homo-sex situation as follows: "You know, Pierre, when the tent was set up and most boys came to have a sleep-out, well, I was the only one not having sex" (Bagley, 1997, p. 185). Without doubt Freud would have been happy to learn about this reality because it would have supported his belief that all individual were capable of acting in accordance to his postulated "bisexuality" norm for humans (a fact Freud recognized possibly because of his knowledge of the Ancient Greek males), and especially because he had also situated homosexuality as the first manifestation of a person's sexual desires that may or may not be acted upon (de Kuyper, 1993).
When I ventured in gay communities in 1978, a major new experience involved the learning about so-called "gay-identified" males, many still being teenagers, and they often were gender nonconformable. As a rule, they had also grown up thinking themselves to be the only ones with homo-sex desires in their neighborhoods, their school, or even in their town or city. Their feelings of isolation had been extreme, resulting in their belief that male homosexuality was exceptionally rare, and many had grown up perceiving themselves to be "freaks." In recent books and papers dealing with gay youth, and on related internet pages, these stories are repeated, and similar life situations were highlighted in the Australian 'Here for Life' Youth Sexuality Project Final Report.
The process of realizing a same sex orientation, and either hiding this or being open, often results in:
damaged self esteem; distancing from family and peers; attempts to avoid disclosure; distortion of nearly all relationships; increasing sense of isolation; and, sense of inferiority and self loathing
This sense of isolation and negative reinforcement has been shown to increase the incidence of mental health issues in young people, resulting in emotional disorders, self harm and suicide. (Goldfram et al. 1999)
My own adolescent environment, however, precluded having such feelings because desires to have sex with other males, and engaging in such joyful activities, resulted only in knowing that I was part of a majority even if, as with masturbation, my sexual activities with other males were to be private acts (Note 4). It is also doubtful, given the information available from Ancient Greece, that adolescents boys of the period would have experienced self-hatred and isolation, with associated suicidal feelings, because they had love and sex desires for older males. If suicidal feeling existed, they would likely have been experienced by a male youth who was being ignored by all older males. Therefore, the reported exceptionally high rate of "suicide problems" for present-day males recognizing their same-gender sexual desires (males who often identify as gay or bisexual) may be a social construction intimately linked to another possible social construction: the increasing rarity of males reporting same-gender sexual desires and related sexual activity in the Western World. As Chauncey (1994) reports on the basis of the evidence:
...in important respects, the hetero-homosexual binarism, the sexual regime now hegemonic in American culture, is a stunningly recent creation (p. 13).
 At
the end of the 19th century, Ellis (1906) reported on
diverse human cultures over time. There were great variations in male
homosexuality, ranging from its widespread nature in Ancient Greece and Rome, to
more rare manifestations such as being a shaman with gender nonconformable
attributes. Many great individual in history had also been homo-sex desiring
males, and homosexuality was reported to be the rule in male prisons. Its extent
in the military was also noted, the evidence indicating that male prostitution
was the rule in some British regiments. Many of these males were in a category
commonly known as "trade," meaning that they were "real men" compared to men who
were "so," as Nilsson (1998) reported the situation to
exist in a Swedish city during the first half of the 20th century. Generally,
the non-real men performed varying sexual services for the working-class
"real men" who were often young, but included men of all ages. Nilsson also
noted that the merchant marine was a common destination for
homosexual-identified males, the implication being that homosexuality was
likely common in navies (Note
5).
At
the end of the 19th century, Ellis (1906) reported on
diverse human cultures over time. There were great variations in male
homosexuality, ranging from its widespread nature in Ancient Greece and Rome, to
more rare manifestations such as being a shaman with gender nonconformable
attributes. Many great individual in history had also been homo-sex desiring
males, and homosexuality was reported to be the rule in male prisons. Its extent
in the military was also noted, the evidence indicating that male prostitution
was the rule in some British regiments. Many of these males were in a category
commonly known as "trade," meaning that they were "real men" compared to men who
were "so," as Nilsson (1998) reported the situation to
exist in a Swedish city during the first half of the 20th century. Generally,
the non-real men performed varying sexual services for the working-class
"real men" who were often young, but included men of all ages. Nilsson also
noted that the merchant marine was a common destination for
homosexual-identified males, the implication being that homosexuality was
likely common in navies (Note
5).
To date, an interesting body of research work has reported that in the first half of 20th century male same-gender sexual activity was much more extensive than during the last third of the century (Nilsson, 1998; Chauncey, 1994, 1985; Dowsett, 1994; Carbery 1992, Brighton Ourstory Project, 1992; Humphreys, 1975; Kinsey et al., 1948). In fact, not all that long ago, about 40 percent of American males had been homosexually active at least at some point in their lives after the onset of adolescence (Kinsey et al,, 1948), but something happened which caused the elimination of the majority of homosexually active males from the world of male homosexuality. Nilsson (1998) supplied the likely explanation for this event occurring in Europe and in other countries with populations of European origins.
Marshall (1981), Newton (1993), and Chauncey (1994) argue that there has been a slow [homosexuality] redefinition process in the western world in this century, from a definition based on 'gender' - a homosexual man desires men because he is like a woman - toward a universal 'sexual' definition: a homosexual man, however "feminine" or "masculine" he is, is homosexual because he desires men... It is interesting that this change, and the concomittant separation of men who were "so" from "real men," occurred at the same time as, and was indeed influenced by, a growing openness of male homosexual life toward and visibility from society.
The "real men" were generally from the working class (the largest segment of population at the time) and some males from this group are described by Minton (1995). "[The two males in a study sample] represented a growing number of working-class young men who migrated to urban centers in the 1920s and 1930s, seeking the "sex trade" as a means of income. As long as their masculinity was not compromised, they had no qualms about engaging in sex with other men." Many of these men, however, did not receive money for their services, although tokens of appreciation were common, and others participated in "trade" for no other reason than the enjoyment Nilsson (1998) and others reported to be the rule for all these "real men." Basically, these men (often teenagers) were well aware that these same-gender sexual activities were infinitely more enjoyable than masturbation, the most common male sexual activity (Munsey, 1997). At a very young age, I had also recognized this fact and, in the neighborhood where I grew up, sanity and altruism also ruled. Most males innately knew (or quickly learned via biofeedback) that masturbation was a selfish act: keeping for yourself what could be shared, and being altruistic was much more enjoyable than being selfish and of questionable intelligence.
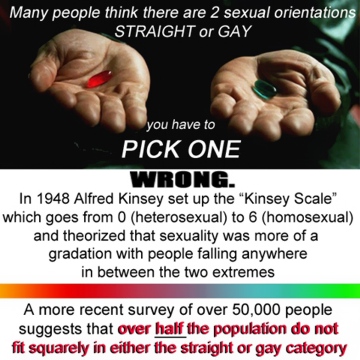
 A
major demographic change has occurred with respect to males participating in
homosexual activity to orgasm since Kinsey et al. (1948)
reported that 37 percent of males had these kind of
experiences since adolescence, with that another
13 percent reporting related desires not acted
upon, for a total of
50% in the study sample reporting some
degree of homosexuality. This is a minimum, however, as Kinsey et al. (1948)
emphasized because, with respect to taboo sexual activities and thoughts,
some males will always withhold such information from investigators no matter
how skilled they may be, and Alfred Kinsey is recognized to have been an
expert in terms of gaining the confidence of interviewed subjects.
Furthermore, for working-class males in the Kinsey sample, the incidence of
homosexuality was higher than 50 percent given that manifestations of male
homosexuality was greatly influenced by social class,
producing incidence differences ranging from 200 to 500 percent, with
working-class males manifesting the highest incidence of homosexual activity
(Note 3).
A
major demographic change has occurred with respect to males participating in
homosexual activity to orgasm since Kinsey et al. (1948)
reported that 37 percent of males had these kind of
experiences since adolescence, with that another
13 percent reporting related desires not acted
upon, for a total of
50% in the study sample reporting some
degree of homosexuality. This is a minimum, however, as Kinsey et al. (1948)
emphasized because, with respect to taboo sexual activities and thoughts,
some males will always withhold such information from investigators no matter
how skilled they may be, and Alfred Kinsey is recognized to have been an
expert in terms of gaining the confidence of interviewed subjects.
Furthermore, for working-class males in the Kinsey sample, the incidence of
homosexuality was higher than 50 percent given that manifestations of male
homosexuality was greatly influenced by social class,
producing incidence differences ranging from 200 to 500 percent, with
working-class males manifesting the highest incidence of homosexual activity
(Note 3).
 Recent
demographic studies, however, have consistently reported lower incidence of male
homosexuality than the Kinsey et al. (1948) results, the
inference often being that the study was seriously flawed. Yet, would similar
data obtained from
Ancient Greek times -
reporting that maybe 100% of male citizens enjoyed (had enjoyed) male
homosexuality activity (probably including love responses in most cases)
- be in error because a modern study of males produced radically different
results?
Basically, the above cited research reporting the
withdrawal of working-class "real men" from the world of male homosexuality
serves to highlight the fact that the Kinsey et al (1948)
data is not wrong.
Instead, it reflects the degree to which male homosexuality existed in
the western world during the first half of the 20th century.
Furthermore, the evidence indicates that extreme homophobic social pressures
were being applied to minimized the extent to which male
homosexuality existed, leading to its increasing rarity - the "freak" situation
- that many gay-identified adolescents have been coding it to be.
Recent
demographic studies, however, have consistently reported lower incidence of male
homosexuality than the Kinsey et al. (1948) results, the
inference often being that the study was seriously flawed. Yet, would similar
data obtained from
Ancient Greek times -
reporting that maybe 100% of male citizens enjoyed (had enjoyed) male
homosexuality activity (probably including love responses in most cases)
- be in error because a modern study of males produced radically different
results?
Basically, the above cited research reporting the
withdrawal of working-class "real men" from the world of male homosexuality
serves to highlight the fact that the Kinsey et al (1948)
data is not wrong.
Instead, it reflects the degree to which male homosexuality existed in
the western world during the first half of the 20th century.
Furthermore, the evidence indicates that extreme homophobic social pressures
were being applied to minimized the extent to which male
homosexuality existed, leading to its increasing rarity - the "freak" situation
- that many gay-identified adolescents have been coding it to be.
The degree of reduction in homosexually active male youth is indicated by Bagley and Tremblay (1998) data obtained via random sampling in Calgary, and then using a highly effective computer technology methodology to solicit information of a sensitive sexual nature, including information about young adult males who had been sexually involved with children (1%) and the ones having related desires (4%) (Bagley et al., 1994). Bagley and Tremblay (1998) reported only 11.2 percent of males had related sexually with at least one other male since the age of 15 years (14.0% since the age of 12 years), and 9.2 percent were currently homosexually active (in the six months preceding the data intake). On the basis of self-identification as homosexual or bisexual (11.1%) and /or being currently homosexual active (9.2%), minus bisexual-identified males who were not currently homosexually active, a study sample of homosexually oriented males (10.9%) was produced and analyzed for a number of attributes to be compared with heterosexually oriented males, including their history of self-harm and suicidality (Bagley and Tremblay, 1997).
An important result of the Bagley and Tremblay (1998) demographic study was support for the hypothesis that flawed methodology was responsible for current demographic studies which had reduced the percentage of homosexually oriented males to one or two percent. The proposed underestimates for these studies were in the range of 400 to 800 percent for homosexuality-related behavior and self-idenfication, respectively. In the same year, the results of the Turner et al. (1998) study, based on a large random sample of 16- to 19-year-old males, confirmed that, on average, a 400% underestimating error could be expected with respect to adolescent males reporting their homosexual activities on pencil-and-paper questionnaires compared to using the computer technology to solicit sensitive sexual information (Bagley and Tremblay 1997, 1998).
The validity of demographic studies using face-to-face interviews or telephone interviews may be inferred by a wise researcher foreseeing what the results would be if middle aged men were asked: "Are you relating sexually with adolescent males, or even younger males." A predictable "zero" (or near zero) percent response to this question would not reflect reality. Although the question requests highly taboo information, underestimates are also predictable if similar methodology is used to solicit information from males who have been homosexually active with males of varying ages. Such behavior remains in a taboo category (still illegal in about 20 American states), and significant underestimates are predictable if confidentiality issues are not addressed in a manner deemed credible by the study subjects who have engaged in such sexual activities (Bagley and Tremblay, 1998).
Unfortunately, face-to-face interviews continue to be used as in the NHANES III study of 17- to 39-year-old males. Only 2.2 percent of males acknowledged having "any male sex partners in their lifetime" (Cochran and Mays, 2000, p. 575), and similar methodologically flawed studies are then cited (given range of study results: "2% to 7%") to conclude that "this is consistent with the prevalence observed in NHANES III" (p. 577), thus creating the illusion of validity for their results. Not mentioned, however, is that this range of demographic results suggests a possible 350 percent underestimating error for lowest results. Instead, it is asserted that "the willingness of men to report same-sex partners in a population-based survey such as NHANES is unknown; thus, the extent to which homosexually experienced men... declared no male sex partners cannot be determined" (p. 577). This assertion, however, is only made possible by not citing studies (e.g. Bagley and Tremblay, 1998; Turner et al., 1998) indicating the likelihood of producing scientifically scandalous underestimates when researchers use highly flawed methodology.
It could therefore be said that, since the Kinsey et al.'s 1948 study, about 70 percent of the males who once enjoyed being homosexually active (most often as adolescents and young adults) were to not to be anymore, apparently because the definition of who was "homosexual' was changing. As Foucault and others noted, homosexuality was taking on a "species" meaning which was also implemented by the American military by 1941 (Purkiss, 1997). Instead of homosexuality simply having been something all males could enjoy, the new "meaning" became infinitely more negative. In addition to the psychiatric decree that all homosexual males were "mentally disordered," many psychiatrists liberally propagated additional negative beliefs about homosexual individuals. Purkiss (1997) summarizes the outcome of (malignant?) psychiatric indoctrination in the American Military:
[In addition to defining homo-sex desiring males to be "inverts," or "like women, military administrators] therefore expanded upon the concept of the homosexual by adding components of violence, immorality, uncontrollable sexual impulses, and a potential threat to society. But woven into these new fabrications were the central ideas proposed by psychiatrists: homosexuals were sick, morally vacant, predatory, and in need of help.
Society - via its law makers - had also decreed that adult males engaging in same-sex sexual activities of any kind were "criminals," and laws had been changing since the early 1880s in Canada and Britain to make sure that all homosexual acts were criminalized, including the intent to engage in homosexual activities, as opposed to only anal sex between males having been a criminal act in the past (Kinsman, 1987). Given these labels and related punishments, the full weight of society's power to define the norms - what is acceptable - was made to apply, especially with respect to male homosexuality. All boys were somehow also being taught that the rejected and often abused easily identifiable "sissy" (the gender nonconformable boy) in early childhood would, by adolescence, be transformed into "the fag," This represents the learned belief that males who are like females must desire other males sexually, thus replicating the "sexual inversion" ideology based on hegemonic heterosexuality: if a male desires another male sexually, he must be a female because only female are sexually attracted to males. As for the supposedly more positive word "gay," the well indoctrinated adolescents almost immediately gave the word a meaning consistent with their acquired beliefs. Goldstein (1999) defines the current definition of the word in reference to the Columbine High School murder / suicide event:
The word "faggot" has never merely meant homosexual. It has always carried the extrasexual connotation of being unmanly [being like a female]. But these days, the implications of that insult have expanded. To say that a certain behavior is "so gay" can apply to anything stupid, clumsy, or outré. It’s probably the most effective way to call a guy a loser, and in this age of sexual candor, when high school students know that some of their peers may actually be gay, the accusation has an even more fearsome ring.
Male Youth Suicide Problems: Worsening Since 1950, Higher Rates for Homosexually Oriented Males, and Greater Risk for Suicide.
The male youth suicide problem for 15- to 24-year-old males increased 3-fold from 1950 to 1990 (Table 1), the increase being the greatest (5-fold) for males aged 15- to 19 years. Since 1950, males have also accounted for 88.5 percent of the additional deaths by suicide in the male and female 15- to 19-year-old category, and 95.5 percent of additional deaths in the 20- to 24-year-old group, meaning that the increase in youth suicides since 1950 has been almost exclusively a male problem. A number of general ideas have been given to explain the increasing adolescent male suicide problem, and Gibson (1989) was one of the first to suggest that homosexually oriented youth may account for about one-third of these deaths, but "some experts rejected the conclusions as being drawn from biased samples" (Remafedi, 1999, p. 1291; Remafedi 1999a).
|
Table 1 - American
Youth Suicide Rates: 1950 to 1990 |
Age Range
(Years)
Suicide Rate
1950
[% Male]
Suicide Rate
1990
[% Male]
Suicide Rate
Increase
[% Male]
15 to 19
M - 3.5
F - 1.8
[66%]
M - 18.1
F - 3.70
[83%]
M: 14.6 ( 5.2X)
F: 1.90 (2.1X)
[88.5%]
20 to 24
M - 9.3
F - 3.3
[73.8%]
M - 25.7
F - 4.10
[86.2%]
M: 16.4 (2.8X)
F: 0.8 (1.2X)
[95.3%]
15 to 24
M - 6.5
F - 2.6
[71.4%]
M - 22.0
F - 3.9
[84.9%]
M: 15.5 (3.4X)
F: 1.3 (1.5X)
[92.3%]
|
M = Males, F = Females, X = Suicide
Rate Increase Multiple. |
 Tremblay
(1995) proposed that up to 50 percent of male youth
suicide deaths may involve homosexually oriented males. This proposal contrasted
with the results from two methodologically flawed postmortem studies (Rich
et al., 1986;
Shaffer et al., 1995) commonly used to suggest that
homosexually oriented adolescents are not at greater risk for suicide than their
heterosexual counterparts (Muehrer, 1995;
Moscicki, 1995). On the basis of suicide risk
indicators, however, including their research results, Bagley and Tremblay (1997a)
speculated that more than half of male suicide deaths may involve homosexually
oriented males. Given that the greatest increase in suicides has been in the 15-
to 19-year-old category, that males form the vast majority of additional youth
deaths from suicide since 1950, and that the greatest amount of male suicidality
information based on sexual orientation criteria for this age group is
available, a survey of the available information and related implications is
warranted.
Tremblay
(1995) proposed that up to 50 percent of male youth
suicide deaths may involve homosexually oriented males. This proposal contrasted
with the results from two methodologically flawed postmortem studies (Rich
et al., 1986;
Shaffer et al., 1995) commonly used to suggest that
homosexually oriented adolescents are not at greater risk for suicide than their
heterosexual counterparts (Muehrer, 1995;
Moscicki, 1995). On the basis of suicide risk
indicators, however, including their research results, Bagley and Tremblay (1997a)
speculated that more than half of male suicide deaths may involve homosexually
oriented males. Given that the greatest increase in suicides has been in the 15-
to 19-year-old category, that males form the vast majority of additional youth
deaths from suicide since 1950, and that the greatest amount of male suicidality
information based on sexual orientation criteria for this age group is
available, a survey of the available information and related implications is
warranted.
The trend in mainstream youth suicidology to assume that sexual orientation factors are not significantly different in suicide rates or suicide problems has created a general lack of awareness that homosexually oriented males may be greatly overrepresented in the worsening suicide problems (Gibson, 1989; Remafedi, 1994; Savin-Williams, 1994; Tremblay, 1995). This assumption persists in spite of the in spite of the Bell and Weinberg (1978) study data indicating that white predominantly homosexual males, by the age of 20 years, were 14 times more at risk for a "first time" suicide attempt than their heterosexual counterparts. Bagley and Tremblay (1997) replicated this factor (to the average age of 22.7 years) for a large random sample of 18- to 27-year-old Calgary males, and a further analysis of the "suicide attempt" data for males 17 to 29 years of age in the Cochran and Mays (2000) NHANES III (National Health and Nutrition Examination Survey) study produced Odds Ratios similar to the two previously noted studies (OR range for the three studies: 12-15, Note 8). Given the average age of the Bell and Weinberg (1978) sample (37 years), the suicidality results for homosexual males best represent the situation existing in the early 1950s. At that time, "first time" suicide attempt incidence to the age of 17 years for white predominantly homosexual males was 4.9% percent: 28/575 (Bell and Weinberg, 1978).
The studies reporting on the suicidality of homosexually oriented male youth have used varied methodologies, thus creating interpretation problems and making it difficult to be absolute about the numbers, but a general trend is apparent from the available data and reported results. The lifetime suicide attempt incidence for homosexually oriented male adolescents has greatly increased over the years (about 6 times) given the Bell and Weinberg (1978) data (a 4.9% "first time" suicide attempt incidence by the age of 17), and the more recent study results. Studies based on varied North American volunteer community samples of gay and bisexual males report lifetime suicide attempt incidences averaging 30 percent (Bagley and Tremblay 1997), with a range of 20 to 42 percent for ten published American studies (Remafedi et al., 1999). These results have also been replicated in school based random sampling YRBS (Youth Risk Behavior Surveys, or similar surveys), and two of these studies specifically report suicidality results for male adolescents based on sexual orientation.
Based on a 1987 Minnesota study of grade 7 to 12 students, Remafedi et al. (1998) report a lifetime suicide attempt incidence of 28.1 percent for males identified as gay or bisexual by the average age of about 15 years, compared to 4.2 percent for heterosexual identified males. Using the same sample data, Saewyc et al. (1998) report that older gay and bisexual male adolescents (15- to 19-years-old) have a lifetime suicide attempt incidence of about 33% by the average age of about 17 years. Garofalo et al (1999) does not specifically give the suicide attempt rate (based on a 12-month period) for males identified as gay, bisexual, and "not sure" about their sexual orientation (GBN), but an estimate of 33 percent was determined on the basis of the information given (Note 6). Other studies (some not yet published, but the data is available) report similar results on average for homosexually oriented adolescents not differentiated on the basis of gender (Table 2).
|
Table 2 - GLB Youth:
Increasing "At Risk" Status |
Survey /
Suicidality Category
Mass 952
GLBN (Gay, Lesbian,
Bisexual, Not Sure) vs
Non-GBLN
Mass 971
GLB* and/or Homo-sex
Active vs
Heterosexual
-Identified
Seattle 951
*GLB-
Identified vs
Hetero-
sexual
Identified
Vermont 952
Males &
Females: Homo-
sex active vs
Hetero-sex
active.
Mass '93
Males & Females: Homo-sex active vs
Hetero-sex
active.
Considered Suicide
46.4% vs
24.6%
1.9-Times3
54% vs
22%
2.5-Times
34.2% vs 16.7%
2.1-Times
59.2% vs
37.1%
1.6-Times
41.7% vs
28.6%
1.5-Times
Planned Suicide
40.5% vs
17.5%
2.3-times
41% vs
18%
2.3-Times
31.1% vs 15.7%
2.0-Times
52.8 vs
28.7%
1.8-Times
29.7% vs
24.5%
1.2-Times
Attempted
Suicide
36.0% vs
8.9%
4.0-times
37% vs
8%
4.6-Times
20.6% vs 6.7%
3.1-Times
40.7% vs
15.2%
2.7-Times
27.5% vs 13.4%
2.1-Times
Medical Care
Associated with
Suicide Attempt
N/A
19% vs
3%
6.3-Times
9.4% vs
2.2%
4.3-Times
26.5% vs
6.2%
4.3-Times
20.0% vs
4.7%
4.2-Times
"Self-Harm"
(Defined4)
Incidence:
"A" VS "B"
?-Times
?-Times
?-Times
?-Times
?-Times
Suicide
Attempt
(Defined4)
Incidence:
"A" VS "B"
?-Times
?-Times
?-Times
?-Times
?-Times
Medical or Psychiatric Hospitalization Associated with Suicide Attempt
Incidence:
"A" VS "B"
?-Times
?-Times
?-Times
?-Times
?-Times
SUICIDES
Incidence:
"A" VS "B"
?-Times
?-Times
?-Times
?-Times
?-Times
|
1. Unpublished Studies - 2. Published Studies but relevant data not given. Information obtained from other sources. 3. **More at Risk Factor for GLB Adolescents Compared to Heterosexual Adolescents.4. Defined by Ramsay and Bagley (1985) and Bagley and Ramsay (1985), and used by Bagley and Tremblay (1997): Note 7 - *GLBN = Gay, Lesbian, or Bisexual Identification; N = "Not Sure." |
Result from Youth Risk Behavior Surveys have also repeatedly indicated that homosexually oriented male and female adolescents are generally more at risk for the more serious suicide behavior: (1) considered suicide, (2) planning a suicide, (3) attempting suicide, and (4) attempting suicide with resulting medical attention (Table 2). In the category of "suicide attempt associated with having received medical attention," it is assumed that, as a rule, the most life threatening suicide attempts, or suicide attempts with a definite intent to die, would have a greater likelihood of resulting in the individual having receiving medical attention, but this may not always be the case, at least for gay and bisexual males (Remafedi et al. 1991).
The YRBS study results listed in Table 2 include homosexually oriented females, and female data tends to reduce major differences existing between males as indicated from the Garofalo et al. (1999) and Remafedi et al. (1998) study results. In the two studies, statistical significance was eliminated between homosexual and heterosexual female suicide attempters in the multivariate analysis, but great differences for suicide attempts incidence were reported for homosexually oriented males compared to their heterosexual counterparts. In the Garofalo et al. (1999) study, LBN females are 2.0-times more likely to report a suicide attempt than heterosexual females, while the factor is 6.5-times for GBN males compared to heterosexual males. In the Remafedi et al. (1998) study, the higher risk factor is 1.4 times for LB females and 7-times for GB males compared to their heterosexual counterparts. Therefore, it is suspected and predicted that an analysis of only the male data in other YRBS studies would likely show more serious suicidal behaviors than their heterosexual counterparts, compared to results generated from the combined male and female data (Table 2).
An indication of the magnitude of differences in suicidality of males based on sexual orientation was reported by Bagley and Tremblay (1997) on the basis of a large random sample of males ranging in age from 18- to 27-years-old. Their suicidality results are presented in two categories of self-harm behaviors based on previous epidemiological studies: "self-harm" (often called suicide attempts by adolescents, but without the intent to die, and the behavior is usually not life threatening), and "suicide attempts" representing a definite attempt at self-killing (Note 7). Compared to heterosexual males, homosexually oriented young adult males were 3 times more likely to report "self-harm" in their lifetime; this is remarkably similar to the reported differences, based on sexual orientation, for "suicide attempts" reported in YRBS studies (Table 2). For strictly defined "suicide attempts," however, Bagley and Tremblay (1997) reported that young adult homosexually oriented males were 14 times more likely to have attempted suicide than their heterosexual counterpart; and the magnitude of risk increases four to five times from their relative risk for for having engaged in "self-harm" activities, to their relative risk for a "suicide attempt" (Note 8).
Homosexually oriented male adolescents are also at risk for serious suicide attempts as reported by Remafedi et al. (1991) from their sample of 137 gay and bisexual male youth ranging in age from 14- to 21-years-old : "Fifty four percent of all suicide attempts (37/68) received risk scores in the 'moderate to high' lethality range." In the 45 attempted suicide cases where the rescuer was not the victim (76% of cases), 58% "received scores in the 'moderate to least' rescuable range. In other words, the predicted likelihood of rescue was moderate to low despite the actual occurrence of an intervention" (p. 871). Unfortunately, since 1991, studies reporting on the suicidality of homosexually oriented youth have only reported "suicide attempts" (with a related analysis) without investigating their degree of lethality, nor were "suicide attempts" rigorously evaluated to separate the ones best classified as "self-harm" from the ones best classified as deliberate attempts to take one's life (Note 7). The Remafedi et al. (1991) and YRBS data (Table 2), however, suggests that maybe more than 25 percent of suicide attempts by gay or bisexual identified adolescent males result in medical interventions, thus indicating a higher likelihood for suicide for these males.
The high proportion of homosexually oriented male adolescents who attempt suicide places them at higher risk for an eventual suicide either as adolescents or later in life (Lewinsohn et al., 1993; Kotila and Lonnqvist, 1989; Sellar et al., 1990; Shafii et al., 1985; Otto, 1972). In this respect, Garland and Ziegler (1993) reported that the "best single predictor of death by suicide is probably a previous suicide attempt" (p. 172). Community samples of homosexually oriented youth have also produced high rates for repeat suicide attempters, six study samples producing a 44.2 percent average for the proportion of gay and bisexual male suicide attempters who became repeat suicide attempters (Table 3), the suggestion being that suicide is an ongoing problem for many of these youth. A similar percentage (39.9%) resulted from the Bell and Weinberg (1978) data, thus indicating consistency in this respect over time. Unfortunately, published studies have not been located on the risk for an eventual suicide by adolescents with a history of repeated suicide attempts. It is possible that such individuals, especially males, are at much higher risk for committing suicide than males with a history of only one suicide attempt.
|
Table 3: - G(L)B Youth
Lifetime "Suicide Attempt" DATA |
STUDY
(N)1 MALES
MEAN AGE
% SUICIDE ATTEMPTERS
REATTEMPT RATE
60
GB Males
20
31.0%
37%
29
GB Males
18.3
31.0%
20%
108
GB Males
20.6
20.0%
45%
137
GB Males
19.6
30.0%
44%
Rotheram Borus, 1994
Visiting Hetrick & Martin
Institute (N.Y.)
138
GB Males
(14-19)
+/- 17
39.0%
52%
902
GLB Youth
(14-21)
+/- 18
30.0%
67%
Means
(6 Studies)
30.2%
44.2%
|
1. A variety of community-based volunteer samples. 2. Sample of gay/bisexual/lesbian individuals with suicide attempt prevalence given for entire group. |
The lifetime incidence of "suicide attempts" for homosexually oriented male adolescents has increased about 6-fold since 1950, from about 5 to 30 percent. Of significant interest are the YRBS study result producing a "suicide attempt" average about about 30 percent for a 12-month period: 32.3% for the 5 studies (Table 2). Given that these rates coincide with lifetime estimates from community samples (Table 3), this similarity likely reflects, at least in part, the possibility that adolescents in school define a "suicide attempt" in a more liberal way; a minor injury may be interpreted to be a suicide attempt. Another possible contributing factor is the high likelihood of homosexually oriented adolescents to be repeat suicide attempters (Table 3). It is important to recognize, however, that the random sampling YRBS studies likely solicits data from a wider spectrum of homosexually oriented adolescents than the representation obtained from volunteer community based samples. If this applies, the suicide problems of homosexually oriented adolescents may actually be more serious than proposed in the worst case hypotheses.
At issue, however, has been their representation in youth suicide problems, and especially their representation in suicide statistics. Mainstream suicidologists have often criticized suicidality results from gay community based samples because of their assumed biased nature (Moscicki, 1995; Muehrer, 1995), and always to counter efforts to have homosexuality issues addressed in youth suicide education and prevention programs where indifference to homosexuality was the rule, as it had been in mainstream youth suicidality research (Remafedi, 1994; Savin-Wiliams,1994; Tremblay, 1995). Tremblay (1995) also suggested that a mean spirited objective had motivated the production of the 1995 Suicide and Life Threatening Behavior special issues on "Sexual Orientation" edited by Muehrer, Moscicki, and Potter (1995) who are from the National Institute of Mental Health (NIMH) and the Centers for Disease Control (CDC).
Tremblay (1995) felt that the document was not created by individuals who really wanted to see homosexuality issues addressed in mainstream youth suicidality education and prevention programs, and that maybe mainstream youth suicidality researchers were not to be encouraged to begin soliciting sexual orientation information in their research. By 1999-2000, this outcome was the ongoing research behavior that the CDC was modeling as a part of its boldly emphasized "Leadership Role." Apparently, the CDC's role is "to ensure the availability of accurate and current information on health risk behaviors among young people, [to provide] funding and technical support to states and major cities to conduct a Youth Risk Behavior Survey" (CDC, 1999), but it is not to model any research behavior such as soliciting "sexual orientation" information from adolescents.
The CDC's official YRBS questionnaire does not solicit "sexual orientation" information (CDC, 1999a), meaning that the CDC does not recognize this factor in adolescent problems in spite of the wealth of information indicating otherwise, nor does the CDC apparently believe that such information should be solicited. Although the questionnaire does solicit information about "sexual intercourse," generally assumed to mean "penis-vagina" sex, anyone thinking the requested information may apply to same-sex sexual intercourse would be in error given the confirmation of its heterosexist definition in Question #63. "The last time you had sexual intercourse, what one method did you or your partner use to prevent pregnancy?" Therefore, to the year 2000, the CDC has continued to ignore "sexual orientation" issues in youth suicide problems, which can have only one result. When any "at risk" group of adolescents are ignored, their concerns are also ignored, and the ones responsible for this are essentially working to maintain a maximum casualty status in the ignored sector of the adolescent population.
In spite of the ongoing modeling of indifference to homosexuality issues in youth problems by the CDC, results from relatively rare school-based studies which had solicited "sexual orientation" were being peer reviewed and published: Remafedi et al. (1998) and Saewyc et al., (1998) for a 1987 Grade 7 to 12 Minnesota student sample, Garofalo et al. (1998, 1999) for a 1995 Grade 9 to 12 Massachusetts student sample; Faulker et al. (1998) for a 1993 Grade 9 to 12 Massachusetts student sample; and Durant et al. (1998) for a 1995 Grade 8 to 12 Vermont student sample. It was only for the Garofalo et al. (1999) study, however, that information was made available to permit an estimate of the proportion of male suicide attempters who are homosexually oriented.
Given the 12-month period 33 versus 5.1 percent attempted suicide rate for GBN (gay, bisexual, and "Not Sure" about their sexual orientation) males forming 4.7% of the male population, it was then possible to calculate that about one quarter (24.3%) of male suicide attempters are in the GBN category (Note 6). Therefore, 4.7% of the students of GBN males account for about 25% of the male suicide attempt problem. Given, however, that the study is based on an amended form of the pencil-and-paper Youth Risk Behavior Survey questionnaire from the Centers for Disease control (CDC, 1999a), and that these surveys likely underestimate the numbers of homosexually oriented individuals by a factor of 3 to 4 (Bagley and Tremblay, 1998; Turner et al., 1998), it is therefore postulated that all homosexually oriented male adolescents, had they been identified by Garofalo et al. (1999), would account for maybe 60 to 80 percent of male suicide attempters. This estimated correction would be consonant with the Bagley and Tremblay (1997) results: 62.5% of young adult male suicide attempters (lifetime incidence) were in the homosexual or bisexual category, defined on the basis of self-identification and/or being currently homosexually active.
The probability that homosexually oriented male youth account for at least 50 percent of suicide attempters, and the fact that these males are more at risk than heterosexual males for the more serious suicide behaviors, such as more serious forms of suicide attempts (Bagley and Tremblay, 1997, 1997a; Remafedi et al., 1991; Table 2), leads to the informed proposition that more than 50 percent of male youth suicides (maybe up to 75 percent) involve males for whom homosexuality issues are, or have been, a significant factor in their lives. It is also known that some males do commit suicide for reasons expressed by Nicolas and Howard (1998) in their study, "Better Dead Than Gay!" and as outlined by Tremblay (1998-1999) in a web page titled "Better to be Dead Than Gay."
Homosexually Oriented Male Youth: Ongoing Suicide Problems?
The Bell and Weinberg (1978) report that, out of 105 homosexually oriented males who had attempted suicide at least once, 62 percent reported that "homosexuality" was associated in their first suicide attempt, a percentage replicated in a 1993 study (Note 9), and 43 percent of these suicide attempts were related to problems in a homosexual relationship. These "first time" attempts were also distributed over given age ranges, with half (52%) occurring by the age of 20 years. Twenty-seven percent (27%) of the attempts had occurred by the age of 17 years, 25 percent between the ages of 18 to 20 years, 27 percent between the ages of 21 and 25 years, and 22 percent after the age of 25 years.
In addition, 39 percent of the male suicide attempters (7% of the sample) were repeat attempters, thus indicating consistency over the last 50 years given that, in recent studies, 44.2 percent of homosexually oriented male youth who attempted suicide (13.3 percent of the sample populations) are repeat attempters (Table 3). The doubling of the percentage of repeat suicide attempters is indicative of increasing ongoing suicide problems, likely of the most serious kind, with implication yet to be studied. My experience in gay communities has revealed that male suicides and suicide attempts remain as a fact of life after homosexually oriented youth have made contact with gay communities. However, researchers have not explored this aspect of the problem, except for Bell and Weinberg (1978) reporting that homosexual relationship problems were associated with about 27 percent of first time suicide attempts.
The Remafedi et al. (1991) study of 137 gay and bisexual male (14- to 21-years-old) reports data indicating that 39 percent of studied youth had been runaways, 39 percent sexually abused, 35 percent arrested, and 20 percent had engaged in prostitution. The associated attempted suicide incidences for males having these often overlapping attributes are 37 (20/54), 47 (25/53), 44 (21/48), and 43 (12/28) percent respectively, the average for the sample being 30 percent. With respect to gender attributes, 23 percent of the males were classified "feminine," 26 percent were "undifferentiated," 31 percent were "androgynous," and 20 percent were rated as "masculine," and their respective suicide attempt incidences are 48 (15/31), 34 (12/35), 26 (11/42), and 11 (3/28) percent. There is therefore a general "suicide attempt" risk decrease from males being feminine, to males being masculine, the former having a 4.4 times greater likelihood for having attempted suicide than their "masculine" counterparts (48% vs 11%).
Many gay and bisexual identified adolescent males with a history of being runaways or throwaways, and especially the ones venturing into prostitution, form a sector of the more visible "gay communities" given that they are relating sexually with homosexually oriented men; Bell and Weinberg (1978) reported that 27 percent of predominantly homosexual males studied had paid for sex, and 25 percent had been paid for sex (p. 311). Not all gay and bisexual male adolescents making contact with gay communities, however, are in these categories, and little had been studied or written about their experiences and problems, including their ongoing risks for suicide problems and suicide. Real life story segment are nonetheless occasionally encountered within the context of researchers reporting on significant problems for which gay and bisexual male adolescents are at risk:
...[Y]outh who received the intervention [a lengthy safer sex education program] said that they would engage in unsafe sex when they felt particularly distressed because they thought it was hopeless for them to protect themselves from becoming HIV positive. In addition, youths who were overwhelmed by emotional distress would bring to the group problems regarding their latest crisis, for example, being involved with a partner who was suicidal or who was being threatened by a previous partner; for these youth these problems took precedence over making behavior changes toward less unprotected sex (Rotheram-Borus, 1995, p. 593).
A significant number of homosexually oriented male adolescents are attracted (commonly enough "only attracted") to older males and they will seek to have sexual relationships with them, often with the hope that love will be a major part of the relationship. This aspiration for love is an integral part of the adolescent male prostitution world, and "many youth" who have ventured into the Los Angeles Youth Service Center are described by Gabe Kruks.
The "sugar daddy" usually present himself to the youth in a loving caretaker manner. For street youth who have a past history of rejection and/or abuse, the promise to be loved and cared for is a compelling one. [These youth usually have many of these relationships and] each of these is a cycle of falling in love, believing that life will now be wonderful forever and that this older adult truly loves the young person, discovering that in fact it is just sex that the adult wants, feeling the impact of one more betrayal, and ending up on the streets again. This whole cycle lasts an average of 1-2 months, and the youth often becomes extremely suicidal at the end of each cycle (Kruks, 1991, p. 518).
Gay and bisexual male adolescents and young adults engaging in prostitution are reported to be at higher risk for suicide attempts (Nicholas and Howard, 1998), but they have not been the only ones attracted to older males and acting accordingly. Others have also been seeking sex (with the hope of love) relationships with older males as illustrated in the special "Love" issue of San Francisco's gay youth XY Magazine:
But when I came out, the closeness I was looking for wasn't what I found. Instead, I fell into the gay community's 'if you're gay, young and cute, you have to be one of those guys who sleeps around' stigma... And I learned from all the wonderful people I met that sex was just sex and that the whole closeness thing was merely a pipe dream - certainly unattainable [if not via sex]... My problem arises when people just coming out see our community as only sexual. That affects me. They learn, like young people in every culture, from their peers and elders. What they see, hear and experience is what they are going to assume the gay community is. With this type of base, they are going to have a very difficult time making their love lives flourish... There are some people who want more than sex and don't feel "sex is just sex" (Weldon, 1997, p. 53).
Marc describes his encounters from the age of 17 when he illegally ventured into gay clubs on a quest to find the males he was most attracted to: the ones about 10 years older than himself.
[By the age of 19, he had] had two "official" relationships... lasting no more than a couple of months, [and he has not been impressed with what he learned.] Maybe this pattern simply indicates bad choices on my part. I guess I can see why older men think 19-year-olds have nothing more than sex to offer. But it surprises me that the older crowd want shallow, detached physical contacts while their younger counterparts are searching so very, very hard for something more substantial (Foster, 1997, p. 21).
The attraction of young gay males for older males is described in the "Older Partner" section of the report, Dangerous Inhibitions: How America is letting AIDS become an epidemic of the young. The section begins with: "Many young people find older partners attractive. All the young men and women participating in one series of PMI focus groups said that they prefer their sexual partners to be at least five years older than them" (Collins, 1997). Rotheram-Borus et al. (1995) reports that "many homosexual male adolescents have sexual relationships with homosexual men..., the group with the highest prevalence for AIDS" (p. 589), but most researchers have not been up front about this reality. For example, the Povinelli et al. (1996) study reports on a sample of 501 males aged 13 to 21 years "who self-identified as homosexual or bisexual or as having sex with men" (p. 33), the implication being that 13- to 16-year-old males are "men." The Remafedi (1994) study sample of 239 males aged 13 to 21 years uses similar terminology. The males in the sample were "self-identified as gay or bisexual and/or had sex with men... High risk sex between men account for the largest proportion of AIDS cases among adolescents (13 to 21 years of age)" (p. 163). More honestly, however, Morris et. al. (1995) reported "that younger gay men with older partners are the leading edge of the [HIV-AIDS] epidemic in their cohort" (p. 24), and this problem would have begun early adolescence for some of the youngest males in the sample who were 18 years of age when studied.
Adolescent males who identify as gay or bisexual at the youngest age are at the greatest risk for suicide attempts (Remafedi et al., 1991; Schneider et al., 1989; D'Augelli et al., 1993; Hershberger et al, 1997; Nicholas and Howard, 1998), and they are most likely to be the youngest individuals becoming associated with some aspect of gay communities such as youth groups from which many study samples are obtained (Schneider et al., 1989; D'Augelli et al., 1993; Hershberger et al, 1997; Proctor and Groze, 1994). For many homosexually oriented male adolescents, however, their first contacts is with a well known part of gay communities known as the "public sex" or "anonymous sex" arena which has been participated in by about 50 percent of gay and bisexual males (Tewsbury, 1996). Uribe and Harbeck (1992) report on the related experiences of adolescent males:
Of the 37 males [in high school ranging in age from 16- to 18-years-old], 35 were already sexually active with other males. The average for the first sexual experience was 14 years, and in the majority of the cases this was with an unknown male... None of the males in this sample had his first sexual experience in a 'safe' manner, and none was still with his first sexual partner. [Furthermore], half of the study participants acknowledged engaging in suicide attempts in the year prior to the interview... Fifteen of these boys were living with friends, two admitted to living with 'sugar daddies,' and three were in residential or foster homes for gay adolescents (p. 21-22).
Family problems, reported to be almost universal for these males, is a factor significantly associated with suicide attempts (Schneider et al., 1989: Nicholas and Howard, 1998). Family problems and lack of services for these adolescents often result in a "lack of support" situation also linked to suicide attempts (Schneider et al., 1989; D'Augelli et al., 1993; Hershberger et al, 1997). Associated factors such as becoming homeless, dropping out of school, stress, and having friends who attempted suicide, have been linked to suicide attempts by gay and bisexual male youth visiting the Hetrick and Martin Institute in New York (Rotheram-Borus, 1994). About 25 to 40 percent of male street youth may be homosexually oriented (Kruks, 1991; Savin-Williams, 1994; Kipke et al., 1995). Runaway youth have elevated lifetime suicide attempt incidences ranging from 15 to 29 percent (Stiffman, 1989; Rotheram-Borus, 1993), and homeless gay youth were estimated to be three times more at risk for suicide attempts than their heterosexual counterparts (Gibson, 1989). One sample of 53 GB male street youth had a 53 percent lifetime suicide attempted incidence (Kruks, 1991).
Remafedi et al. (1991) reported high rates of sexual abuse for gay and bisexual male youth (39%), but also noted that sexual abuse generally postdated sexual identification as gay or bisexual. The unspoken implication is that the sexual abuse likely occurred after they made themselves available for sexual experiences often occurring via making contact with some gay community attribute such as the "public sex" arena, as most of the first sexual experiences occurred for the teenage gay males studied by Uribe and Harbeck (1992). Sexual assault and rape after adolescent males have made contact with gay communities, however, remain hidden in all studies reporting such experiences, often assumed to be "child sexual abuse" having occurred before the individual made contact with gay communities. This assumption may be incorrect.
About 20 to 39 percent of homosexually oriented males have experienced unwanted sexual acts (sexual abuse, sexual assault) by the age of 17 (Doll et al., 1992; Caballo-Dieguez and Dolezal, 1995; Holmes, 1997, Lenderking, 1997, Remafedi et al., 1991), and such experiences have been linked to a lifetime higher incidence of suicidal behaviors, including suicide attempts, in adolescent and young adult males (Bagley et al., 1994; Bagley et al., 1995), and in young adult gay males (Nicholas and Howard, 1998). The international incidences for boys being sexually abused ranges from 2 to 11 percent, with up to 16 percent results in Alberta, Canada (MacMillan et al., 1997). Homosexually oriented males may also be at greater risk for sexual abuse at younger ages given that one study reported that boys sexually abused before the age of 13 were 4 times more likely to be homosexual than boys not sexually abused (Finkelhor, 1979).
Substance abuse is also associated with suicide attempts of gay and bisexual male youth (Remafedi et al., 1991), as is alcohol abuse (D'Augelli and Hersberger, 1993), and both these problems are well recognized risk factors for both suicide attempts and suicides in mainstream youth populations (Brent, 1995; Mazza, 1997). Youth Risk Behavior Survey studies have reported that homosexually oriented adolescents (self-identified as gay, lesbian, or bisexual and/ or being homosexually active) are many times more at risk for multiple drug and/or alcohol use and abuse than their heterosexual counterparts (Garofalo et al. 1998; Faulkner et al., 1998; Note 10). Psychiatric symptoms such as depression have also been linked to suicide attempts for homosexually oriented youth (Nicholas and Howard, 1998; Hershberger et al, 1997; D'Augelli et al., 1993), and depression has been linked to suicide attempts and suicide in mainstream adolescent and youth population (Brent, 1995; Mazza, 1997). For homosexually oriented adolescents, however, psychiatric symptoms are likely related to, or exacerbated by, many of their most unfavorable life outcomes, and these symptoms should not be deemed "biological" in origin.
The Seal at al. (2000) qualitative study of seventy-two 16- to 25-year old young men who have sex with men (YMSM) from two midwest American cities reports on the multifaceted socially imposed problems of these youth. "Low self-esteem and self-worth, a lack of self-care and self-love, hopelessness and depression and teen suicide factors were believed to underlie unsafe sexual behavior:
There are time when I wished to God I would have just been dead. I couldn't go through the pain of who I was or the pain of trying to live my life. There was so much hurt. It wouldn't have mattered if I had gotten HIV. To be that would have been the simplest solution. I wouldn't have had to do a thing. I just would have had to lay there. I wouldn't have had to slit my wrists or commit suicide any other way. It's a more painful way, but if you're on a suicide mission it doesn't matter.
Participants further pointed out that may YMSM, and particularly YMSM of Color, lived with a pervasive sense of hopelessness in multiple aspects of their lives. Consideration of adverse long-term consequences of behavior was difficult for men who lived with daily violence, poverty, and despair and who held few expectations about a lengthy life:
When it comes down to it, the guys I talk to just don't care about life. They say life has nothing to offer them. A lot of times their mothers and fathers have disowned them and their family won't deal with them anymore because they are gay. They have no life, no family no future (p. 10).
...Some YMSM derived excitement from conscious unsafe sex: 'There's times with anonymous pickups that I won't use a condom. The thrill of not knowing whether he (an anonymous pickup) is gay or straight makes it difficult for me to stay safe.' Several respondents reported that more and more YMSM found sexual excitement in the 'Fuck of Death', that is, conscious unprotected receptive anal sex with a known HIV-positive partner or 'bug giver'" (p. 11).
An association between a history of suicide attempts and practicing unsafe sex by gay males was reported by Lewis (1988), but individual cases of gay males contracting HIV as a way to commit suicide had been reported as early as 1985 (Frances et al., 1985; Flavin et al., 1986). By the late 1990s, the phenomenon was reported in association with gay youth (Tompkins-Rosenblatt, 1997: "Intentional HIV contraction: implications for direct child and youth care"), and from an analysis of Vancouver's Vanguard Project cohort of young men who have sex with men ranging in age from 18 to 30 years. A history of attempting suicide was the second most statistically significant association differentiating males who were "risk takers" compared to males who were not risk takers with respect to placing themselves at risk for contracting HIV (Martindale, 1997). Seal et al. (2000) report a similar phenomenon as noted above, but another factor is apparently also associated with desires for death by young men who have sex with men (YMSM):
They [YMSM] figure that they will have as much fun as they can now because they see old guys sitting in Venue X who like 40 and 50 and 60 years old and who haven't done anything with their life. Or, if they have, they're single and sitting in Venue X hitting on the young guys. The [YMSM] figure if they die young they wouldn't have to worry about that. It's the fear of age that many kids don't want to face - that they will get old. They figure that they have do do lots of things before their beauty fades (Seal et al., 2000, pp. 10-11).
In a Salon magazine interview, Edmund White commented on the gay community ageism factor possibly implicated in a conscious desire to contract HIV as a form of suicide, which could also be more unconscious for some gay males:
If you say you're going to be dead by 40, they say, "So what? There's no gay life after 40, anyway." Especially in France, but even here. You can easily be a gay in his 20s and never meet a gay over 40 because you don't see them in the bars. They don't go out, they're not part of your world, and if you do see them, you consider them pathetic (Reitz, 1997).
The above data basically renders a part of the story related to suicide problems for many homosexually oriented male adolescents, with one high risk attribute likely being an important factor in early identification as gay or bisexual, possibly dropping out of school, and venturing into the identifiable parts of gay communities at an early age. This common attribute of gay and bisexual identified male adolescents is a high level of "femininity" which, on the basis of mutlivariate analysis, resulted in "feminine" males having a 3-times greater risk for a suicide attempt than their counterparts (Remafedi et al., 1991).
Feminine Males: A Social Construction of Suicide Problems
In the recent history of homosexuality in the western world, there has been an association between males who identify as homosexual or gay and high levels of femininity (Ellis, 1906; Purkiss, 1997; Chauncey, 1994; Minton, 1995; Nilsson, 1998). The acquired perception was that males who desired the "female role" when relating sexually with other males (being passive: permitting a penis to penetrate oneself) were 'homosexual," or "inverts" because they assumed the sex role of the opposite gender. These males were also believed to have a degraded status compared to sexually dominant males, and the ideology was rooted in the sexist perception that anything "female," and especially the sexual role of being penetrated by a penis, was a status very inferior to the status of "men" who had a long history of proclaiming and enforcing their supremacy status vis-à-vis females.
By the middle of the 20th century, however, there was a significant exodus of homosexually active males - the males who had been sexually dominant with sexually passive males - from the world of male homosexuality existing in European societies and in societies with population primarily derived from European countries. This recent socially constructed world of male homosexuality therefore produced an predictable outcome. Males who are generally the most feminine became overrepresented in the world of male homosexuality, this being the opposite of the situation existing in the first half of the 20th century.
Bell et al. (1981) reported that gender nonconformity was the single most statistically significant difference between predominantly homosexual males and predominantly heterosexual males, and the reason for this association is evident from their data on the "self-ratings" by males (as they were to the age of 17 years) using a "highly feminine to highly masculine" 7-point Likert scale (Table 4). Although rating on the scale overlap for homosexual and bisexual males, there are major differences, especially with respect to high femininity scores: 28 percent of homosexual males classified themselves in the three highest levels of femininity, compared to only one percent of heterosexual males, and the latter also only placed themselves in the least feminine of the three categories. In the two highest "masculine" ratings (5 and 6), 67 percent of heterosexual males classified themselves as such versus only 18% of homosexual males.
|
Table 4 - Bell,
Weinberg, and Hammersmith (1981) |
F-M Rating/
Male Groups
0
Feminine
1
2
3
4
5
6
Masculine
Homosexual Males
N = 575 : Percent
02
08
18
30
25
13
5
Heterosexual Males
N = 284 : Percent
0
0
01
07
24
42
25
|
F-M Rating/
|
.........Feminine: 0 - 3........ |
Masculine: 4 - 6 |
|
Homosexual Males
|
58% |
43% |
|
Heterosexual Males N = 284: Percent |
8% |
91% |
|
Remafedi, Farrow, and Deisher (1991) |
F - M
Category
..Feminine..
Undifferentiated = 26%
Androgynous = 31%
.Masculine.
% of Males
in Category
23%
(31/137)
26% + 31% = 57%
(35/137) / (42/137)
20%
(28/137)
Attempted
Suicide %
48%
(15/31)
Undifferentiated = 34%
Androgynous = 26%
(23/77 = 30% )
11%
(3/28)
Bell et al. (1981)
Homosexual Males
Approximated
10%
72%
18%
The distribution of homosexual males on the Bell et al. (1981) masculinity to femininity scale produced a similar distribution to the one resulting form the Bem (1974) gender classification used by Remafedi et al. (1991) for their sample of 137 gay and bisexual male youth ranging in age from 14- to 21-years-old (Table 4). For this study, the incidences of suicide attempts associated with each category were then used to determine the Odds Ratio at a 95% confidence interval for a suicide attempt by gay and bisexual male youth who had sufficient femininity attributes to warrant a classification other than "masculine." The more feminine gay and bisexual males, representing 82% of the sample in the feminine, androgynous, or undifferentiated categories, are 3.2 times more likely to attempt suicide than their "masculine" counterparts: Risk Ratio = 1.1 < 3.2 < 9.8 (Note 11). This is basically the same result reported by Remafedi et al. (1991) on the basis of multivariate analysis for the risk of a suicide attempt based on "feminine gender roles" (p. 873).
The association of femininity in males with being homosexually oriented as adults was also reported by Green (1987) in the book Sissy Boy Syndrome. The 44 "feminine" boys studied over many years became young adult men with a 75% probability of being gay or bisexual, as rated by the Kinsey 0-6 fantasy / behavior scale. A control group of 35 "conventionally 'masculine' boys" had only one young adult male in the bisexual category (p. 99-101). It should not be assumed, however, that all "feminine" boys will be homosexual or bisexual given that 25% of feminine boys in the Green (1987) study were heterosexual. On the basis of the Bell et al (1981) data on self-rated masculinity to femininity levels of males when they were children and adolescents (Table 4), and assuming that predominantly homosexual males make up about 5 percent of the population, 58 percent of the males in the 0-3 category would be homosexual (42% heterosexual), but homosexual males form 100% of the two highest - "0" and "1" - feminine categories.
Feminine boys have a long history of being abused in sexists societies and their reported higher risk for suicide problems would be, in part, induced or exacerbated by the ongoing abuse they have been subjected to since early childhood. Although Eric Rofes (1995) is describing his own childhood below, he is also describing a variation of the childhood and adolescent lives of numerous gay males I have met over the years.
I knew I was queer when I was a small child. My voice was gentle and sweet. I avoided sports and all roughness. I played with the girls... Heresy was a boy who cried a lot when he got hurt..., a boy who couldn't throw a baseball..., a boy putting on girls' clothing. Heresy was me. As I got older, and fully entered the society of children, I met the key enforcer of social roles among children... He was... like an evil spirit entering different bodies in different occasions... In any group of three of more boys, the bully was present.
I know a lot about bullies. I know they have a specific social function: they define the limits of acceptable conduct, appearance, and activities for children. They enforce rigid expectations. They are masters of the art of humiliation and technicians of the science of terrorism. They wreaked havoc on my entire childhood. To this day, their handprints, like a slap on the face, remain stark and defined on my soul...
As I entered adolescence... I saw other sissy boys become neighborhood toughs. They formed gangs of bullies that tormented us... Watching the powerless take on the trappings of power, I would shake my head and withdraw into deeper isolation... The abuse I suffered in American public schools, from kindergarten to my senior year of high school, created deep psychic scars with which I have struggled throughout my lifetime.
These same scars are shared by many others. We will never forget that we were tortured and publicly humiliated because we refused to be real boys, acted "girlish," or were simply different. This was the price we paid for being queer. (Rofes, 1995, pp. 79-80)
The operating principle underlying this wholesale abuse of males with any degree of visible femininity is a perception acquired by very young boys as the result of careful social teaching / indoctrination. Most of them, in fact, are still growing up with perceptions reflecting the historical male-imposed status of females as inferiors to males, and the outcome was summarized by Mandel (1996) in the doctoral study abstract. The study explored, via 200 interviews with adolescent girls and boys in an American middle school and junior high school, some important adolescent gender identity issues in North America.
First, this study suggests that students’ assumptions about heterosexuality perpetuate a norm of heterosexuality and constrain adolescent gender identity. Not only do students believe that a heterosexual identity is central to their gender identity, but stereotypic notions about femininity and masculinity largely inform their beliefs about who they are and who they cannot be... Students’ descriptions of masculinity are also stereotypic and are largely defined by an anti-feminine norm. Unlike the ways in which girls can and do value masculinity, boys do not and cannot value femininity.
Second, this study asserts that there is a social and sexual curriculum in the culture of middle and junior high schools by which girls and boys construct their gender identities. This heterosexist curriculum, it is argued, perpetuates gender role stereotypes, limits gender identities, empowers masculine boys and disempowers girls, less masculine boys, lesbians, and gay males. The most pervasive indicators of this curriculum - due to heterosexism - are illustrated in the amount of gender disrespect, peer sexual harassment, homophobic language, and the highly (hetero)sexualized nature of adolescent gender relations in these middle and junior high schools. (Mandel, 1996)
When "boys do not and cannot value femininity," they have basically acquired the age-old perceptions many human groups often acquired of other human groups firmly believed to be one's inferiors. Therefore, the many boys who still often say something like 'Yuk! Girls! I'm not playing with them!" are essentially a replication of the well taught white highly racist boys who not long ago would have said: "Yuk! Niggers! I'm not playing with them!" In other words, contemporary boys are still learning to have a intense hatred of femininity (females) which is evidenced by their hatred for - and abuse of - boys deemed to be "like females," meaning that they actually hate humans who are 100 percent females. Rofes (1995) notes that, with respect to the current use of the word "gay" as an epithet by adolescents, "the links to youthful misogyny are evident" (p. 81). Suzanne Pharr, in her 1988 book "Homophobia: A Weapon of Sexism," describes outcomes of such abuse continuing into adulthood:
What is unhealthy - and sometimes a source of stress and sickness so great it can lead to suicide - is homophobia, that societal disease that places such negative messages, condemnation, and violence on gay men and lesbians that we have to struggle throughout our lives for self-esteem... It is not by chance that when children approach puberty and increased sexual awareness they begin to taunt each other by calling these names: "queer," "faggot," "pervert." ...It is at puberty that the full force of society's pressure to conform to heterosexuality and prepare for marriage is brought to bear. Children know what we have taught them, and we have given clear messages that those who deviate from standard expectations are to be made to get back in line. The best controlling tactic at puberty is to be treated as an outsider, to be ostracized at a time when it feels most vital to be accepted. Those who are different must be made to suffer loss. It is also at puberty that misogyny begins to be more apparent... (Pharr, 1993).
It is not, however, only in schools and in peer groups that adolescents males with detectable feminine attributes have been abused more than males without these attributes, or males who are effective at hiding such a part of themselves. Homosexual males are more likely to report having been assaulted by parents than heterosexual males, and effeminate homosexually active adolescent gay and bisexual males have been the most at risk for such assaults (Harry, 1989). Homosexually oriented adolescents are also at risk for not being tolerated and even being rejected in their families (Pilkington and D'Augelli, 1995; Telljohann and Price, 1993). One study of 221 GLB youth (lifetime suicide attempt incidence = 40.3%) reported family problems to be in second place, after the youth's self-perception, with respect to significant associations with the risk for a suicide attempt (Proctor and Groze, 1994).
Modern gay identified adult males often have a history of childhood gender nonconformity and, as older adolescents, young adults, and older males, their average higher levels of femininity compared to average heterosexual males has been significant, as based on my more than 20 years of communicating with many gay males and soliciting many life histories. Rofes (1995) reports similar observations:
...[I]nterviews with gay men of all classes, races, and educational backgrounds reveal a strikingly large percentage who acknowledge a sissy past when asked. This is true of gay men who exemplify American ideals of masculinity, as well as hypermasculine men in the gay ghetto. Some sissy boys grow up to be nontraditional adult men - androgynous, "effeminate," transgendered, or simply gentle - while others transform themselves into traditional versions of masculinity... Some gay men have talked and written candidly about their struggles as sissy boy [with many example of this fact of life supplied] (p. 81-2).
Rofes (1995) was most troubled about the "sissy boy" reality being ignored not only in mainstream society but also by gay and lesbian individuals advocating for an end to the wholesale abuse of their adolescent counterparts. In this respect, he emphasized that "to say sissies = gay male youth is considered offensive by many in the gay community" and suggested "that little attention has focused on the plight of the sissy [because] gay male activists and educators alike carry unresolved feelings about their own sissy pasts... These barriers must be examined, challenged, and overcome because - regardless of future sexual orientation - sissy boys have become contemporary youth's primary exposure to gay identity" (p. 81).
This outcome, however, may not occur in the immediate future, for reasons imbedded in parts of Bradley Boney's 1996 paper on the "sissy," himself having in this category:
In August of 1993, the following appeared in the Denver Post: "Sissy boy Johnny Roy Hobson runs with his arms up and his toes turned in. He prances, minces and pouts. In short, he's so annoyingly effeminate you just want to slap him" (Dillard-Rosen, 1993) Although the critical reception of Bonin-Rodriguez's work has been overwhelmingly positive, these three sentences from Sandra Dillard-Rosen's review of Talk of the Town represent the type of sissy-bashing that proceeds from the dangerous impulse to erase "negative stereotypes" from queer representation without first interrogating how and why they were first constructed as "negative."
Sedgwick (1993) takes up this issue in in an essay titled, "How to Bring Your Kids Up Gay: The War on Effeminate Boys," which she demonstrates how the effeminate boy has been positioned as the "haunting abject" of both gay, and the larger hegemonic culture. The latter is disturbing enough, but the discomfort with which so many gay men approach the sissy boy continues to perpetuate a discourse of self-loathing, considering those studies which have found that a large number of adult gay men at least perceive the sissy boy to be a part of their history. Sedgwick explains how this effeminaphobia is coupled with the legitimate gay project of unraveling gender and sexuality to debunk the notion that anyone "who desires a man must by definition be feminine [and vice versa]" (p. 157). In light of such studies, she concludes that
"the eclipse of the effeminate boy from adult gay discourse would represent more than a damaging theoretical gap; it would represent a mode of annihilating homophobic, gynephobic, and pedophobic hatred internalized and made central to gay-affirmative analysis. The effeminate boy would come to function as the discrediting open secret of many politicized adult gay men" (p. 158) (Boney, 1996, pp. 54-55. Referencing changed by author.)
Many gay males with a history of being sissies have been living out the demands of not being who they were / are, for approval reasons, often because they want others gay males to desire them sexually. Boney (1996) reports on this all too common reality as he has lived it, but he continues to struggle with the repression / denial of his inner "feminine" self.
Today, I have been surprisingly successful at erasing the sissy from my own body. I have employed the technology of the gym with amazing results. I drive a motorcycle and buy clunky, construction-worker-type boots in an attempt to push the limits of "masculinity." I still live in constant vacillation between championing my inner sissy child (for he so often comes shining through) and hiding him from view in order to increase my currency in the gay market. As much as I constantly check it, I am sometimes guilty of the sissy self-loathing I rail against. So I ask myself, what is so discomforting about a nellie boy? If, as Dillard-Rosen states, Bonin-Rodriguez produces an effeminate character "that some gays may find stereotypical and offensive," what is the basis of that offense?
The discomfort of both Dillard-Rosen and the gay men for whom she claims to speak is, I believe, fundamentally misogynistic. Our culture continues to view the feminine as less-than and ultimately valueless. We deal the best we can with the "natural" feminine attributes of women, but we do not wish effeminacy on our sons. I don't know how to explain to a fabulously effeminate gay man that his corporeal style is an offensive stereotype. In the end, I don't know how to explain that to myself. (pp. 55-6)
This rabidly misogynous anti-sissy situation (sissy-bashing, which becomes self-bashing so that one has access to sexual partners) in North American gay communities has also been reported by others, such J. Michael Bailey, a researcher of homosexuality. In his summary of his research available on his web pages he notes that:
Consistent with past research, we have found that gay men are strongly prejudiced against feminine men as sex partners. ...[O]ur research [Bailey et al., 1997] would suggest that feminine gay men, in particular, may be most likely to suffer rejection from other gay people. In addition to their mistreatment by heterosexual people, we might expect that they would have more adjustment problems than most (Bailey, 2000).
The expression "adjustment problems" may be an understatement, and I think there is something savage and suicidal about a community which has been waging a war against an attribute so much a part of its members' individual identities. This community attribute may also be especially deadly for the more feminine gay male adolescents who venture into its midst, especially after they have spent a lifetime being abused in the mainstream world because of their detectable "feminine" attributes. In the final analysis, what Boney (1996) has managed to do with his "femininity" is exactly what the bullies in public schools - the "masters of the art of humiliation and technicians of the science of terrorism" (Rofes, 1995, p. 80) - had not been able to do, and same applies for the misogynous efforts of even more lethal highly sexist bullies (therapists) with feminine boys who also bravely resisted their professional forms of anti-sissy terrorism. Basically, these bullies decreed that males must be masculine, and the more stereotypically masculine one is - as in making this possible by working out in gyms - the better! Gay community ideology therefore reflects the ideology (and then some) of all who sought to harm gender nonconforming boys as they grew up, meaning that many gay-identified males do eventually identified with their abusers, have become abusers, and they are now essentially working to harm the boys who are as they once were: unacceptably feminine.
About 80 percent of gay or bisexual identified adolescent males and young adults venturing into gay communities have varying levels of often detectable "femininity," with about 25 percent being "feminine" (Remafedi et al., 1991). These males have also been at high risk for suicide attempts (35%), the highly "feminine" males having the highest risk (48%), compared to "masculine" gay and bisexual males (11%). However, their venture into gay communities will often be a shock, and a common complaint often voiced by adolescent gay males - the ones with integrity who thought they could now be honest after a history of having to lie for survival reasons - was stated as follows by one such male: "Why do so many lie all of the time." This fact of life applies as much to sugar daddies as if does to average gay males, and one French ethnomethodology study reached a similar conclusion. Most gay and bisexual males lie in one or more ways when meeting each other with a "sex" (maybe "love") objective in mind:
The majority of homosexual males I have met would rather not know the truth (in spite of their professed desire to know the truth)... The very frequent use of lying by cruising homosexual males sometimes causes problems. For example, after sexual pleasure is experienced a love (passion) response may result. Is a relationship possible? Based on what? Being blind? In fact, when we are relating with an entrenched liar, there are no rational ways to detect where the lie end and where truth begins (de Luze, 1990: Conclusion - Translated by author. Original text in Note 12).
One of the ways gay males lie, of the many ways listed in four major categories and 34 subcategories, is via in their appearance, and "muscles" headed the list of eleven ways gay males lie physically. One case presented is similar to the self-reported life story of Bradley Boney (1996) after he ventured in the gay community, coded what was desired by other gay males if he wanted to have sexual partners, and altered himself accordingly. Guy is a 23-year-old male with an "effeminate" adolescent history which had earned him the "fag" label. To counter this aspect of himself, he eventually became muscular to appeal to other gay males, but de Luze (1990) discovered the truth about Guy:
Guy's muscles are a desperate effort to make others believe that he is a real male sure of himself and morally sound, while he is in fact a timid male with a complex of problems, very nervous, and perpetually anxious; this became evident as the evening progressed and alcohol was giving him confidence and making him talkative. The evening ended with Guy reporting that he is constantly depressed and that he has already attempted suicide three times (de Luze, 1990: Mensonge du Paraître: Muscles - Translated by author. Original text in Note 12).
The extent that lying by appearance - via muscular development - exists in gay communities is unknown, but some gay males believe what Scott Thompson of "Kid in the Hall" fame noted in a Salon Magazine interview: "...the sissy is the truth. The muscle queen is not. That is a false construct held up by wires, strings, steroids and the gym. It's not real. And if gay men aren't going to accept the sissy, then they're doomed" (Morgan, 1998). Harris (1991) described the situation and some implications:
One would have anticipated that gay liberation... would have significantly changed the way that our culture views effeminacy, providing a new protective environment in which to experiment with unconventionally masculine forms of behavior. A central paradox of the birth of the subculture, however, is that in resisting the effeminate stereotypes and gestural paradigms that have tyrannized gay men of the past, we have created a new Frankenstein - the "good gay," masculine, assimilated, forceful, deliberate... In liberating themselves from effeminacy, homosexuals have taken on yet another albatross, accepted more, not less rigid notions of how they should express their homosexuality, and essentially invented - to borrow a stereotype ridicules in the black community - the gay oreo, effeminate on the inside, masculine without. In the final analysis, liberation has liberated homosexuals into a new totalitarian attitude towards their mannerisms, a new contempt for effeminacy... (Harris, 1991, p.76). ...rather than endorsing effeminacy, gay liberation has led to the institutionalization of its ridicule (Harris, 1991, p.78)
In the past few years, my immersion in death via suicide has taught me that individuals not permitted to "be" themselves may end up experiencing serious problems, often of the suicide kind. Many homosexually oriented adolescents are living this reality via having a part of their minds socially programmed to hate their well recognized same-sex desires, and some of these youth do commit suicide, thus acting out the concept "Better Dead Than Gay" (Nicholas and Howard, 1998; Tremblay 1998-99). The inability to "be" who one "is" also results from external pressures which, for all boys manifesting a "feminine" self, is operating via "the bully" and his allies: average adolescents, teachers and other adults who, though their silence, tacitly give their approval to the "masters of the art of humiliation and technicians of the science of terrorism" (Rofes, 1995, p. 80).
A potentially dangerous outcome of the gay community's anti-feminine ideology, however, would be to have some of its anti-feminine members become involved with adolescent suicide prevention, and especially with any part of a mainstream suicide prevention programs targeting at risk gay or bisexual identified male adolescents. To my knowledge, only one such program has been implemented in the world as part of a national suicide prevention strategy: Australia's 'Here for Life' Youth Sexuality Project. In the Final Report for the project, the section "Performance Indicators: Summary of Results" contained the following:
Feedback from young people on resources: Very positive feedback on booklets: simple text; photos & quotes by real young people; no stereotypical gay imagery; do not reinforce “coming out” constructs, pressures or present experiences as homogenous. 5,000 referral fliers distributed - high demand for re-print (Goldflam, 1999).
In producing the booklets, decisions were made by many involved with the project, and it was thought best to have "no stereotype gay imagery" in the booklets, which may mean not having representations of males of the recognizable "feminine" kind. Experience in gay communities, as well as the related data, indicates that about 30 percent of the "most at risk" boys would be "feminine," followed by the remainder being "feminine" enough to not permit their placement in the category least at risk for suicide problems: "masculine" homosexually oriented males (Remafedi et al., 1991; Table 4). Throughout the 'Here for Life' Youth Sexuality Project Final Report, the concept of gay stereotypes is occasionally noted, always with the implicit assumption that the existence of stereotypes is a problem.
Young people with same sex attraction, whether or not they identify as lesbian, gay or bisexual, grow up very aware of the prejudice, discrimination and possible violence they will face if their peers and family discover their sexual orientation. Cultural homophobia is often internalized, thereby reinforcing feelings of marginalization and alienation. The turmoil most people pass through during their teen years is greatly compounded by prevailing negative stereotypes, lack of information, invisibility of sexual orientation and lack of positive community attachment experiences.
The prevailing apparently "negative" stereotype for homosexually oriented male youth is their assumed "femininity," the identifiable attribute resulting in their high risk for abuse since kindergarten, as reported by Rofes (1996). Many boys apparently grow out of their "sissy" status, possibly as a result of related self-hatred rooted in the learned extreme sexism manifested by most boys, but other boys "bravely" refuse to deny their "feminine" selves no matter what the punishments inflicted on them. This outcome is possibly related to valuing femininity, although they may eventually assimilate of the trapping of stereotype masculinity as both Guy (de Luze, 1990) and Bradley (Boney, 1995) did because of gay community misogyny: the dislike and rejection of males who are feminine, which is the dislike (hatred?) of what the majority of these males may be. Problems related to "stereotypes," and especially the more recent "masculine" gay stereotype, are described by Brown (2000; Note 13):
The images we did not want to dominate were what were seen (from Western Australia's point of view) as the “Sydney Look” – the beefed up, ‘good looking’ gay man with short / shaved hair, white shirt, tight jeans etc. The body beautiful image. We did not totally exclude anyone who looked this way, but were keen for it not to dominate as it had in previous strategies. We actively looked for a broader range of young men and women. We wanted to include a range of both masculine and feminine looking young men and women, as well as a diversity of cultural / ethnic
backgrounds... Criticisms of the final images being “too warm and fuzzy” and “they all look about 20” we felt were quite valid.
It would therefore appear like the imagery did not exclude anyone, but it also was not representative of the dominating more feminine aspects of gay male youth. Related problems are noted:
Certainly from an agency and funder point of view, there was a real assumption and pressure that tried to generalize or conform the experiences of same sex attracted youth. You know the line “Oh not all gay men are effeminate therefore gay men are OK” and of course the "if they did not behave so effeminately they would not get so harassed". This was RAMPANT! Its hard to know really how successful the project was in affirming the diversity of same sex attracted youth experiences and lives. There is always room for improvement and room to be challenged (Brown, 2000).
There are many problems to address when tackling gay and bisexual male youth suicide issues, a "critical point" according to Brown (2000) being the issue raised in this paper: Given the distribution of suicidality in the Remafedi et al. (1991, Table 4), we could ask: Is the suicide problems a "sexual orientation" issue, or it is really a "sissy" (i.e. gender nonconformity) issue? And if "we" do not tackle that issue, can we honestly say that we are addressing the GB adolescent male suicide problems?
I felt the term homophobia and even heterosexism have never really adequately explained the environment, and are often only thought of in relation to their impact on same sex attracted youth, rather than youth generally. When homophobia and heterosexism reveal themselves as anti-"sissy" actions or behavior, is this the same as being anti gay? Maybe yes / maybe no. The men's health movement in Australia has tried to tackle these issues, in the context that they impact on all men, and society generally. Part of me feels that if it is only targeted by Gay / Lesbian projects, then the focus on only sexual orientation may continue by default (Brown, 2000).
The 'Here for Life' Youth Sexuality Project was one of the first attempts to tackle sexual minority suicide issues, and much remains to be learned in this respect. An emphasis of the project was on the representation of diversity, meaning that an emphasis was not placed on the overrepresentation of the most "at risk" more feminine gay and bisexual identified male adolescents. One emphasis, however, was on "positive community attachment experiences," as a positive outcome for these youth, but "community attachments" may not be all positive, especially for the more feminine gay and bisexual male youth. In addition, for a significant number of homosexually oriented adolescent males, their "community attachment experience" have occurred via prostitution which placed them at higher risk for depression (Earls, 1989: 70% gay and bisexual males in sample) and suicide problems (Nicholas and Howard, 1998), but these males were apparently not specifically targeted by the project.
The fate of a group of such boys in Sidney is reported in the article "Silence is where the hate grows: silence = death" written in reference to mainstream suicidology having avoided "homosexuality" issues in adolescent suicide research and prevention work:
Although Casey {with a history of eight suicide attempts] reckons he "always knew" he was gay, he became one of the kids who was "forced into doing it". After moving to Sydney, Casey was drawn into a string of abusive "relationships".
Because of his low self-esteem borne of the silence, Casey says he was easy pickings for deeply-closeted homosexual "sick tickets" who found more pleasure in hearing screams for mercy as they held knives to the throats of other parents' sons than in real and open love.
Starved of real love and left with little hope, Casey, like many young gays, turned to chemical "friends" to fill the void. His only human friends became the other youngsters traded by the "sick tickets".
"Of the thirteen of us, I'm one of only three that's still alive today," Casey says. "Most of my friends blew their heads off, some of them OD'd and some of them have died from AIDS. They were all bright kids with talents and promising futures" (Clatcher, 1997).
Homosexually oriented male adolescents at high risk for suicide problems have a cluster of at risk attributes such as being "feminine" to significant degrees, using drugs and alcohol, and running away from home which is often associated with street life and adolescent prostitution. The Here for Life' Youth Sexuality Project, however, did not specifically focus on these attributes in their advertising imagery given the valid criticism that the final images were “too warm and fuzzy” and that “they all look about 20.” One potentially negative result of these images is that at risk youth not leading "warm and fuzzy" lives may not identify with the images, thus leaving them with the feeling that their life issues are not recognized and that help may not be available to them.
There are also many potential problems to be considered by all contemplating the formation of sexual minority youth groups, and little has been written on the subject. Often enough, as noted in the Final Report of the Here for Life' Youth Sexuality Project, the tendency of sexual minority youth to form cliques may sabotage the more ideal objectives of a group. Brown (2000) commented on this issue as well as others:
Your points about boundaries within youth groups, particularly in relation to sexual behavior and also emotional connections / expectations that young people can have. I think we all know that a facilitator (or other group members) does not have to have sex with a group member to damage them!
In relation to better a bad group than no group question... I fall more on the side of better no group, as long as there is someone they CAN talk to. The assumption that you get a group of young people together and automatically there will be a positive, functional, uplifting experience is incorrect - but exactly why it works sometimes and why it can completely be a disaster at other times has yet to be shown to me conclusively. There are just so many variables.
When I compare the guidelines and responsibility for the programs back in 1994 when I first started being involved, to now - 6 years later - there is very little resemblance. There has been an enormous improvement, but still room for more. However to detail the changes and what seemed to work / not work would take some doing - and I fear would be distorted by time and memory. No matter how much we try - there is always that tendency to imagine that what we have now is sooooo much better, and then five years further down the track we will probably look back and say the same thing.
However, what we do have in relation to a number of ways that young people can report, inform, or otherwise make it known that they are not happy with the way things are operating is significantly better. Be it young people getting a bad deal, forced to conform, sexual pressure, or other sorts of unwanted influence from facilitators or other group members. Much of this is around supervision / support and engagement.
I am not that convinced about the long term sustainability of youth groups without a structured backup, support and supervision. I feel many groups place too much pressure on young volunteers, and can place them in too "powerful" position without the capacity to deal with this. I mean - the number of so called trained, adult social workers who have really failed miserably in this respect always astounds me - let alone the position some young people are placed in (Brown, 2000).
My own experiences with a sexual minority youth groups in Calgary from 1991 to 1996 has taught me to give warnings with respect to anyone contemplating the referral of a youth to such a group, especially with respect to accountability and honesty issues. For example, trouble in Calgary's gay community began after I had been reporting some unwelcome "community" truths, such as the reality of adolescents boys relating sexually with much older gay males because they often were only attracted to older males, and about boys ending up in gay clubs by the age of 14 years as a result of their contact with the gay and lesbian youth group. I also reported realities such as an 1994 observation made by a 19-year-old Calgary gay youth leader. On the basis of his experiences with many gay youth groups in Canada, about half were reported to be "fuckfest" (sic) groups. He noted this, however, only after I reported what I had overheard a Calgary Gay Lines peer counselor tell a teenager who had called for advice. He was told not visit the gay and lesbian youth group because he would only get "fucked there" (sic).
The comment made to the teenager was then reported to the one responsible for Gay Lines and to the new youth group leader, a Vietnamese friend of mine who wanted to change things so that positive outcomes would result. I was then told that this sexual exploitation of youth by youth (usually of younger youth by older ones) was an open secret, and that the older gay and lesbian community leaders had done nothing about the situation. I also wrote about the sexual use and abuse of at risk gay youth by older males, including their risk for being raped as it had happened to many interviewed gay males (Note 14); one well known bisexual suicide victim, Bill Clayton, was sexually assaulted at the age of 14 years by a 20-year-old gay or bisexual identified male claiming to be a member of a gay and lesbian youth support group, and Bill had become very suicidal as the result of this experience (Clayton, 1997-2000). Addressing such issues, however, was precluded by the community ideology related to not airing "dirty laundry," meaning that serious problems will remain unacknowledged and ongoing, including the "gay community" problems of the more feminine gay and bisexual males, and the problems adolescent boys experience in gay communities which often deny their presence and the relationships they often have with significantly older gay-identified adult males. The youngest Calgary case I reported on was 12 years of age when he began having a series of such relationships with adult gay males to the age of 17 years when he was interviewed. Bell and Weinberg (1978) reported that 25% of predominantly homosexual males studied, after they had reached the age of 21 years, had had male sexual partners 16 years of age or younger (p. 311).
In 1997, a longtime Calgary gay community leader was reading the comments (complaints) made by Weldon, (1997) and Foster, (1997) with respect to their experiences of only being sexually used by older gay males as quoted above. The community leader immediately labeled these responses to be "homophobic," meaning that if anyone does not accept gay community males as they are - a significant number being users, abusers, and liars - and if your are not happy with the situation and maybe even become suicidal as the result of these repeated negative experiences, you will then be branded "homophobic." A similar response would surely apply if the most "feminine" gay and bisexual male adolescents and young adults began complaining about what many gay communities have become ideologically, and if they also reported on the related varied abuses inflicted on them by their own kind.
Research Proposals For The Twenty First Century
Homosexually oriented adolescent and young adult homosexually oriented males are at risk for suicide problems. This fact is reflected in HIV-related cohort studies reporting high rates of major depressive disorder (MDD) in adult gay male psychiatric histories (Atkinson et al., 1988; Williams et al., 1991; Rosenberger et al., 1993; Perkins et al., 1994; Dew et al., 1997). These studies and the Bagley and Tremblay (1998) study have nonetheless reported normal rates of current depressive mental health problems for adult gay males, and the same applies for one sample of HIV-positive and HIV-negative African-American men (Peterson, 1996). For a larger similar sample of African-American males, however, elevated current rates of depression were reported (Richardson, 1997), and Schneider et al. (1991) reported that 30 percent of gay men studied experienced suicidal ideation within a 6-month period.
Adult gay males also have psychiatric histories characterized by elevated rates of drug and/or alcohol abuse (Atkinson et al., 1988; Williams et al., 1991; Rosenberger et al., 1993; Johnson et al., 1996; Dew et al., 1997). These problems seem to be eventually overcome (Bux, 1996), but McKirnan and Peterson (1989) do report higher levels of current alcohol problems for gay males, and the same applies for a large sample of African-American gay and bisexual males (Richardson et al., 1997). Given that adult gay males apparently have elevated rates of personality disorders (Perkins, 1993; Johnson, 1996) and neuroticism (Kelly et al., 1998) that is an indicator of certain personality disorders, and that a link exists between personality disorders and alcoholism (Morgenstern et al., 1997), a subgroup of adult gay males with significant substance abuse problems may exists. Bailey (1999) comments: "Homosexual people are at a substantially higher risk for some forms of emotional problems, including suicidality, major depression, and anxiety disorder. Preliminary results from a large, equally well-conducted Dutch study [Sandfort et al, 1999] generally corroborate these findings" (p. 883).
One reason for this result, however, may be also related to other subgroups of homosexual males, one example being "celibate homosexual males. " They form about 15 percent of the homosexual male population and they have been reported to have ongoing problems (Bell and Weinberg, 1978), including elevated rates of current depression (Bagley and Tremblay, 1998), and a part of their problems may be related to the gay identification process. Not having passed the "tolerance" stage in the coming out process (the next stage is self-acceptance) is associated with mental health problems in adulthood as reported in one study of 196 adult gay and bisexual males (mean age = 28.8 years). The most significant discriminator on a psychological well-being scale (with twice the F-ratio of the next most significant measure, p less than .0000) was the greater suicidality scores of males still at the "tolerance" stage (Brady and Busse, 1994).
Adult gay males are also at risk for experiencing minority stress which, in part, may be related to their high likelihood for having experienced psychological and physical abuse in society (Herek et al., 1997). Stigmatization-related negative life events predict psychological dysfunction in gay men (Ross, 1990), and "minority stress" negatively affects their mental health, increasing their risk for suicidal problems (Meyer, 1996). Much is therefore unknown about adult homosexually oriented males with respect to mental health issues and suicidality, and the same applies for the resolutions of problems from the high risk period of adolescence and young adulthood to middle and old age.
A variety of studies are therefore needed
to answer many of the questions related to homosexually oriented males, their
mental health, and suicide problems over their lifespan. However,
recommendations in this paper are generally restricted to adolescent and young
adult males. Some research projects could also include older males given that
related information is needed to compare with results from studies of
contemporary youth. I am in agreement with Remafedi's (1999)
emphasis on the need for "[p]rospective, longitudinal studies...
[required] to examine the evolving risk of suicide across the lifespan of
homosexual persons." He also noted that "although the understanding of gay,
lesbian, and bisexual youth suicide is increasing, many questions remain
regarding sex and ethnic differences, predisposing social and psychiatric
conditions, protective factors, and constructive interventions" (p. 1291).
Remafedi concluded that "[f]uture population-based surveys should routinely
inquire about sexual orientation to retest prior findings in diverse settings"
(p. 1291). Unfortunately, the history of ignoring homosexuality issues in
mainstream research of almost all human problems continues to be the rule.
Youth Risk Behavior Survey Data Sets
There are, however, low cost research projects which could be immediately undertaken, especially with respect to existing YRBS (Youth Risk Behavior Survey) data sets which have solicited homosexuality information from adolescents in public schools (Table 5). In the listed studies, students were asked questions in one or two of the following three categories:
1. Sexual Orientation - Identification as gay, lesbian, bisexual, or heterosexual, or are they unsure about their sexual orientation.
2. Same-Gender Sexual Activity - Usually defined as having "sexual intercourse" with an individual of one's own sex.
3. Harassment Based on Homosexual Orientation - The question may be: "Have you ever been threatened or hurt because someone thought you were gay, lesbian, or bisexual?" (Wisconsin, 1997), or something like "In the past 30 days, what were you harassed about? (If more than one reason, what was the most upsetting or offensive to you?) Possible Answers: a. I was not harassed; b. Race or national origin; c. Unwanted sexual attention or comments; d. Perceived sexual orientation (gay/lesbian/bisexual); e. Physical disability; f. Other not listed; g. Don't know why I was harassed. (Oregon, 1997)
|
Table 5 - Youth Risk
Behavior Surveys / |
Information Solicited /
Data Sets
1
Self-
Identification
GLBN
2
Same-Gender
Sexual
Activity
Subjected
to Anti-
Gay Abuse
Related
Published Papers
Yes
Mass '93
Yes
Faulker et al., '98
Mass '95
Yes
Yes
Mass '97
Yes
Yes
Mass '99
Seattle '95
Yes
Yes
Vermont '95
Yes
Durant et al., '98
Vermont '97
Yes
Vermont '99
Yes
Wisc '97
Yes
Oregon '97
Yes
Oregon '99
Yes
Yes
SF '97
Yes 3
|
1. All Youth Risk Behavior Survey Studies, except for Minnesota (1987):
"Minnesota Adolescent Health Survey Questionnaire") and Connecticut (1997):
"Voice of Connecticut Youth Survey" Results available from
SSCW, 1999). |
The data generated by these questions, given the information also solicited about other problems (e.g. suicide attempts, varied forms of drug and alcohol use), permits the exploration of significant associations between individuals deemed to be homosexually oriented (gay, lesbian, or bisexual identified, possibly including the ones unsure of their sexual orientation) and other negative outcomes that can be compared to the results for heterosexually oriented individuals. Although published and unpublished studies have reported homosexually oriented adolescents to be at significantly greater risk for many negative life events (e.g. various drug and alcohol usage: Note 10), not one YRBS study has explored the data sets via Multivariate Cluster Analysis to produce a more holistic perception of the at risk situation for homosexually oriented adolescents, and the same applies for community based studies of these youth.
All YRBS which have solicited self-identifying "homosexuality" information from adolescents (self-identification as homosexual, gay, lesbian, or bisexual and/or engaging in same gender sexual activity) have reported a greater likelihood for "suicide attempts" by homosexually oriented adolescents (Table 2), and especially by homosexually oriented males when the data was analysed on the basis of gender. Although adolescent males attempt suicide at rates about one-third that of females, they are about 4-times more likely to commit suicide (Garland and Ziegler, 1993), thus indicating major suicidality differences based on gender. Given these differences, plus the fact that the relative likelihood for a suicide attempt between homosexually and heterosexually oriented individuals is much higher for males than it is for females (Garofalo et al., 1999: 6.4-times versus 2-times; Remafedi et al., 1998: 7-times versus 1.4-times), all statistical analyses must therefore be done separately for males and females, and results reported accordingly. It has long ago been established that individuals with serious problems, such as alcoholism, should be separated on the basis of both sexual orientation and gender for analysis. A factor may be significantly associated with lesbian problems but not with gay male problems, and combining gay males and lesbians for analysis may reduce the factor to statistical insignificance (Tuite and Luitan, 1986).
For homosexually oriented male youth, variation in their relative likelihood for having suicide problems, compared to heterosexual males, may also be related to other factors such as illegal drug use and abuse, having been sexually abused, or other variables, but such statistical analyses have not been done with YRBS data sets. Their greater likelihood for a suicide attempt may also be specifically generated for more than one variable, for comparisons with heterosexual adolescents, or for comparisons with other homosexually oriented male nonattempters, as done by Remafedi et al. (1991). This study, however, only reported greater likelihood of a "suicide attempt" on the basis of individual variables, leaving inquisitive students wondering if suicide attempts are even more likely for individuals having more than one risk factor in their histories. Real life situations involving suicide problems are generally holistic in nature, with many problems factoring into events such as suicide attempts, suicide attempts associated with having received medical attention, and suicide.
The available YRBS data sets could therefore produce an exceptional study summarizing the risk status of homosexually oriented students based on self-identification and/or being homosexually active, inclusive or not of the ones unsure about their sexual orientation. Those who are unsure about their sexual orientation may be treated as a separate population. The study would also report on the effects of harassment based either on one's known or assumed homosexual orientation, thus producing results not only for homosexually oriented adolescents who are harassed, but for adolescents not sure of their sexual orientation, and for the ones claiming to be heterosexual but are targeted for similar harassment. An unrecognized and unresearched major factor in such harassment is gender nonconformity existing in individuals who may be heterosexual identified, gender nonconformity being the underlying reason motivating the abuse of sissies in elementary schools. Sissy boys, however, often become the ones targeted for anti-gay harassment in junior and senior high schools and a longitudinal study reported that gender nonconformity in preschool ("behaviors that are counter to typical gender norms, such as aggressive behavior in females and dependence in males") was one of the "early gender-specific risks for suicidal ideation" in adolescence (Reinherz et al., 1995).
With respect to adolescent suicide problems, the importance of harassment on the basis of sexual orientation is made apparent from the Seattle (1995) YRBS data (Table 6). Gay, lesbian, bisexual adolescents (known or assumed to be homosexually oriented), and heterosexual adolescents who were subjected to harassment based on their assumed "homosexual orientation" are at about equal risk for attempting suicide (20.5% and 20.3%). These incidences represent a 4-times greater likelihood for a suicide attempt in the past 12 months compared to heterosexual identified adolescents not targeted for such abuse and having a suicide attempt incidence of 5.5 percent..
|
Table 6 - Suicide Attempt Results
Based on Sexual Identity |
CATEGORIES
Heterosexual
Not Targeted*
N = 6664
89.6% N
Heterosexual
Targeted
N = 449
6.0% N
GLB** Not Targeted
N = 214
2.9% N
GLB
Targeted
N = 110
1.5% N
Suicide Attempters***
Percent Incidence in each Category and
[Percent of All Suicide Attempters]
5.5%
380/6664
[71%]
380/535
20.5%
92/449
[17.2%]
92/535
19.1%
41/214
[7.7%]
41/535
20.3
22/110
[4.1%]
22/535
Suicide Attempters: Associated Medical Attention - Percent Incidence in each Category and [Percent of These Suicide Attempters]
1.7%
113/6664
[62.8%]
113/180
8.6%
39/449
[21.7%]
39/180
7.8%
17/214
[9.4]
17/180
9.6%
11/110
[6.1%]
11/180
Percent of Attempters
in the Category of Seeking or
Requiring Medical Attention
29.7%
(113/380)
42.4%
(39/92)
41.6%
(17/41)
50.0%
(11/22)
|
*Was Target of
Offensive Comments or Attacks Re:
|
In YRBS studies, it would also be important to report the proportions of suicide attempters who are homosexually oriented, as Bagley and Tremblay (1997) did. They reported that 10.9 percent of homosexual and bisexual males accounted for about 25 percent of young adult males reporting lifetime "self-harm" activities, and these males also accounted for 62.5 percent of males reporting a serious suicide attempt. The same should be done in YRBS studies, with a bonus possible when harassment data is solicited for individuals harassed because of their known or perceived homosexual orientation.
From the 1995 Seattle YRBS data (Table 6), GLB adolescents, forming 3.4 percent of the student population, account for 11.8 percent of suicide attempters, and 15.6 percent of suicide attempters reporting that receiving medical attention was associated with their attempts. However, "the homosexuality factor" in the form of "harassment based on perceived homosexual orientation" is also associated with suicide attempts by heterosexual identified adolescents, the group having suicide attempt incidences equal to that of GLB adolescent. It could therefore be said that "the homosexuality factor" is associated with about 30 percent (29%) of adolescent suicide attempters, and 40 percent (37.3%) of suicide attempters reporting that receiving medical attention was associated with their suicide attempts.
For such results, however, given that some
homosexually oriented adolescents were not identified in this study (the ones
who were homosexually active but did not identify as gay, lesbian, or bisexual),
that the ones "not sure" about their sexual orientation were eliminated from the
data analysis, and the high likelihood that many homosexually oriented male
adolescents (maybe up to 75 percent) are likely to not report identification
information on a pencil-and-paper questionnaire (Turner et
al., 1998), the previously noted estimates would be minimums. These
estimates, stated as minimums, are also extremely significant for educators
needing quantitative results permitting the recognition of a very significant
factor in youth suicide problems, and especially in the more serious forms of
this problem.
Youth Risk Behavior Survey: Standardizing Question
Students of youth suicidality based on sexual orientation would greatly appreciate some standardization of question related to sexual orientation in Youth Risk Behavior Surveys which solicit relevant information. Given the current social construction of sexuality in the western world, suggestion in this respect are:
Sexual Orientation
1. How would you describe your
sexual orientation or desires?
|
A. heterosexual
|
B. homosexual |
C. bisexual
|
|
D. unsure
|
E. None of the above. |
Sexual Behavior
1. In the past 5 years, I have
related "sexually" with... ("had sex with"), and you may chose more than one
answer.
|
A. Opposite sex Individual(s) less than five (5) years younger or older than me. |
B. Opposite sex individual(s) more than five (5) years older than me. |
C. Opposite sex individual(s) more than five (5) year younger than me. |
|
D. Same sex Individual(s) less than five (5) years younger or older than me. |
E. Same sex individual(s) more than five (5) years older than me. |
F. Same sex individual(s) more than five (5) year younger than me. |
2. In the past year (last 12
months), I have related "sexually" with... ("had sex with"), and you may chose
more than one answer:
|
A. Opposite sex Individual(s) less than five (5) years younger or older than me. |
B. Opposite sex individual(s) more than five (5) years older than me. |
C. Opposite sex individual(s) more than five (5) year younger than me. |
|
D. Same sex Individual(s) less than five (5) years younger or older than me. |
E. Same sex individual(s) more than five (5) years older than me. |
F. Same sex individual(s) more than five (5) year younger than me. |
3. During the past 3 months, with
how many "same-sex" individuals did you relate sexually (have sex with)?
|
A. I have never had sex with same-sex individuals. |
B. I have had same-sex sexual experiences, but not during the past 3 months. |
C. One (1) person. |
D. Two (2) people. |
|
D. Three (3) people. |
E. Four (4) people. |
F. Five (5) people. |
F. Six or more people. |
4. Questions similar to #3 could be asked of all students to determine the number of lifetime sexual partners of either gender.
Gender Conformity
One's gender nonconformity is very much related to harassment by peers in schools and in society. It is also related to homosexuality, in the popular imagination, and to some degree with the reality of homosexuality as it exist in the modern world. Gender nonconformity, at least for males, is also related to suicide problems. The following question solicit relevant information will produce data which may be important in the understanding of students reporting to have a number of problems.
1. Some boys may be very feminine (like girls) and some girls can be very masculine (like boys). Choose one description in the following list - from "very feminine to "very masculine" that "you" think best describes you.
A. Very feminine.
B. Feminine.
C. A little more feminine than masculine.
D. As much feminine as masculine.
E. A little more masculine than feminine.
F. Masculine.
G. Very Masculine
2. For Boys to Answer: When you were in grades 1 to 6 (Elementary School), you may have been told that you were too feminine and you were even called a "sissy" or other names meaning the same thing. If this happened to you, which one of the statements below best describes what happened to you?
A. I was never called such names.
B. I was called such names only a few times.
C. I was called such names often enough.
D. I was often called such names but by only a few students.
E. I was often called such names by many students.
3. For Boys to Answer: When you were in grades 7 to 9 (Junior High), you may have been told that you were too feminine and you were even called "gay," "fag," or other names meaning the same thing. If this happened to you, which one of the following statements below best describes what happened to you?
A. I was never called such names.
B. I was called such names only a few times.
C. I was called such names often enough.
D. I was often called such names but by only a few students.
E. I was often called such names by many students.
Questions similar to #2 and #3 would be developed for girls considered to be "too masculine" and called related names.
A Boyhood Gender Nonconformity Scale developed by Hockenberry and Billingham (1987) and later modified by Phillips and Over (1992) could be used to measure the past "femininity" status of boys, but corresponding items for females need to be developed given that a similar gender nonconformity scale for girls does not appear to exist.
Suicidal Behavior
In addition to the suicide related questions in the CDC (1999) Questionnaire (No. 22 - 26), the following question would permit a more comprehensive data set related to suicide issues specified to be unknowns in Table 2.
Last 12 Months:
1. If you attempted suicide during
the past 12 months, and an attempt resulted in a visit to a hospital, how long
were you in the hospital?
|
A. I did NOT attempt suicide in past 12 months. |
B. A few hours, but not one full day. |
C. One (1) to two (2) days. |
|
D. Three (3) days to seven (6) days. |
E. One (1) to two (2) weeks. |
F. More than Two weeks. |
2. If you attempted suicide during
the past 12 months, did you receive counseling or therapy related to your
suicide attempt from a psychiatrist, psychologists, or other qualified person
such as a school counselor, social worker, etc.? If so, how long did the
counseling last?
|
A. I did NOT attempt suicide in past 12 months. |
B. Less than one week. |
C. More than one (1) week but less than one (1) month. |
|
D. One (1) to three (3) months. |
E. One (3) to three (6) months. |
F. More than six (6) months. |
3. If you attempted suicide during the past 12 months, which of the following would best describe how you really felt at the time?
A. I hurt myself, but I knew I was not going to die.
B. I hurt myself, but knew I was not going to die. I did it because I wanted to tell someone I needed help, or because I wanted to get needed attention.
C. I hurt myself and did not want to die, but what I did almost caused my death.
D. I really wanted to die, but I knew it would not happen. I knew what I was doing would not kill me.
E. I really wanted to die, and I was sure that what I did would kill me.
Suicide Behavior Before a Year Ago:
1. Your were asked if you attempted suicide in the last 12 months, and you may or may not have done this. Did you attempt suicide before a year ago?
A. Yes, I did attempt suicide before a year ago.
B. No, I did not attempt suicide before a year ago.
Following these question would be a set of
three questions nearly identical to the three questions asked for a suicide
attempt in the past 12 month. The questions would begin with: "If you
attempted suicide before a year ago,..." and would be preceded by the CDC
questions 23-25 rewritten to apply to this time period. The data resulting from
these questions would likely be priceless in terms of obtaining lifetime suicide
attempt incidences, determining the severity of suicide attempts, and the
individual's intent to die.
Youth Risk Behavior Surveys: Error Determination
A serious problem in demographic research that includes sexual orientation questions is the general absence of a subset of behavior related questions for those who self-identify as bisexual or homosexual that are based on the acknowledgment of related sexual desires and/or manifestations of related desires based on varying degrees of participation in - and enjoyment of - same-gender sexual activities. When questions of this kind are asked, using face-to-face interviews telephone interviews, the underestimation in reported behaviors is estimated to range from 200 to 800 percent, based on study by Bagley and Tremblay (1998) who used computer technology methods to solicit taboo sexual information from young adult males.
In the same year, Turner et al. (1998) reported on the effectiveness of using computer technology (including the use of headphones) for soliciting taboo information from a large randomly selected sample of males aged 16 to 19 years. Using pencil-and-paper methodology produced a 400 percent underestimate (on average) for male reporting same-gender sexual activity compared to results obtained from using computer technology, and high underestimates were also reported for other taboo behaviors such as the varied use of illicit drugs.
Such underestimates will likely negatively affect statistical correlations between homosexually oriented adolescents and taboo at risk behaviors such as illicit drug use, and it would therefore be in the interest of all relying on YRBS data and related statistical correlations, including the CDC, to know about the likely underestimates existing in previous YRBS studies, and especially the underestimates for the proportion of students who are homosexually oriented and would have revealed this fact about themselves if flawed data-intake methodology had not been used. It is therefore proposed that YRBS studies using computer technology methods be done in Massachusetts to establish an error estimate for the homosexuality data and related statistical correlations reported in the previous YRBS studies done in Massachusetts.
The supplementary questions listed above
should also be incorporated in the study because the information should produce
improved descriptions of adolescent suicide problems, and a better understanding
of suicide problems based on sexual orientation and associated behaviors. In
addition, the data will permit an improved understanding of suicide issues
related to adolescents reporting harassment and abuse based on one's assumed
homosexual orientation and/or one's perceived gender nonconformity, the two
often being related issues. Exploring associations of the number of sexual
partners of either gender (for a 3-month period, and in one's lifetime) with a
number of other problems is also important given the greater "at risk"
associations reported by Durant et al. (1998) for
homosexually active adolescents compared to their heterosexual counterparts who
had four or more sexual partners in a 3-month period.
Mainstream Population Sampling
Mainstream population sampling is done by researchers wishing to explore certain human realities, often in subpopulation, and they wish to avoid possible bias problems associated samples of self-selected individuals; such criticism were made by Moscicki (1995) and Muehrer (1995) with respect to suicidality results from volunteer samples of gay and lesbian individuals who were closely associated with the more visible parts of gay communities. Mainstream study population may be truly random, or near-random as Bagley and Tremblay (1997, 1998) obtained via stratified random sampling methods. On the basis of such sampling, they were able to demonstrate and confirm that homosexually oriented young adult males have been at significantly greater risk for suicide behaviors in their life histories, and even more at risk for engaging in serious suicide attempts (Note 8).
Random telephone dialing techniques also produce apparently representative study population, and demographic results may be significantly different from the composition of gay community samples commonly used in studies. This outcome was reported by Harry (1990) and summarized in the abstract:
[N]ational probability sample of [American] males interviewed by telephone and asked their sexual orientation. Of these males 3.7 percent reported that they were homosexual or bisexual. Homosexual / bisexual men were compared with heterosexual ones on the demographic variables. This sample produced larger numbers in those groups which appear to be underrepresented in the usual samples drawn from the gay world. These groups include those with little education, married men, older men, minorities, and those living in small towns. It is suggested that probability samples which do not draw directly or heavily from the gay world for homosexual respondents obtain a broader sampling of those having homosexual feelings or behaviors (p. 89).
Harry (1989) reported that 38% of the sampled male population self-identified as homosexual or bisexual was not Caucasian, compared to 18% for heterosexual males, and the same overrepresentation of gay and bisexual males from racial minorities (non-Caucasian) also the result of an 1998 Exit Poll. People of color formed 32 percent of the sample versus an 18 percent representation in the general population, with 4 percent of the sample identifying as gay, lesbian, or bisexual (HRC, 1999). Such results are important for researchers to know, especially with respect to recognizing that gay community samples represent a subset of the total population of homosexually oriented males in society. Telephone sampling, however, only produce study samples of individuals willing to reveal their homosexual orientation to someone requesting the information, and a significant percentage of homosexually identified individuals may withhold relevant information: about 60 to 70 percent of them if the Bagley and Tremblay (1998) homosexual and bisexual identification result for young adult males (11.1%) is accepted as a reasonable approximation of reality. Furthermore, more sensitive "identification" information, such as having engaged in same-sex sexual activity, is often not solicited, thus not permitting the identification of individuals who have been homosexually active but are not identifying as homosexual, gay, lesbian, or bisexual.
Reasonably representative study samples are birth cohorts commonly used in longitudinal studies, as it was done in New Zealand where sexual orientation information was solicited from the subjects at the age of 21 years (Fergusson et al., 1999). As a result of soliciting such information, researchers confirmed that GLB (gay, lesbian, and bisexual) individuals were more at risk for having certain mental health problems. At a 95% confidence interval, homosexually oriented youth were reported to be 6.2 times (CI, 2.7 - 14.3) more likely to have reported a suicide attempt. They were also 5.9 times (CI, 2.4 - 14.8) more likely to be classified as having experienced two or more psychiatric disorders, thus confirming the overrepresentation of homosexually oriented youth in "suicide attempt" problems and in diagnosed psychiatric conditions. Another similar study from New Zealand is being prepared for peer review publication and it will report suicidality results based on gender related sexual attraction (sexual orientation). Distinctions may be made between self-harm and suicide attempts as it was done in the Bagley and Tremblay (1997) study (Note 15).
Study cohorts used for longitudinal studies are obtained via varied sampling methods, and study results are produced by controlling for certain demographic variables such as age, sex, gender, education level, etc.. These samples are generally taken to study specific problems, and the purpose of the CARDIA Cohort is embodied in the name: The Coronary Artery Risk Development in Young Adults. At baseline (1985-86), the sample consisted of an enrollment of 5,115 young adults, 18 to 30 years of age and, about ten years later, a decision was made to solicit "homosexuality" information to investigate of health effects possibly associated with experiencing anti-gay discrimination (Krieger and Sidney, 1997). The male demographic results based on "ever having a same-sex sexual partner" (Table 7: 15.3% for male) was similar to the Bagley and Tremblay (1998) 14.0% percent result for young adult males in the same category. The CARDIA Cohort study reported only slightly fewer females (13.3%) who reported having at least one sexual partner.
|
Table 7 - Cardia
Cohort: Lifetime Same-Sex Partners |
Race/Gender:
White/Black Men
White/Black Women
Total:
Men/Women
Sex of Sexual Partner
N = 693
N = 1031
1,724
Only Same-Sex
Weighted %
5.7% & 0.5%
(5.2%)
1.8% & 0.7%
(1.7%)
3.5%
Both Sexes
Weighted %
10.6% & 5.4%
(9.7%)
12.3% & 5.8%
(11.6%)
10.6%
Total
Weighted %
n = 90
(15.3%)
14.1% & 6.6%
(13.3%)
14.2%
|
*Calculations by author, assuming a U.S. population of only white and black individuals, with about 90% Caucasian and 10% African-American individuals. The results are therefore a reasonable "approximation" of the percentage of white and Black American individuals who report having had lifetime same-gender sexual experiences. |
From the CARDIA Cohort, about 5.2 percent of young adult males could be classified "homosexual" given their history of exclusive same-sex partners, a result consonant with the Bagley and Tremblay (1998) report that 5.6 percent of males self-identified as homosexual. The remaining 8.8 percent of males (14% minus 5.6%) reporting lifetime same-sex partners since the age of 12 years in the Bagley and Tremblay (1998) study also replicates the CARDIA Cohort 9.7 percent of males reporting to have been behaviorally bisexual.
Study samples used in longitudinal studies
are one of the inexpensive ways that important information may be obtained to
better understand the part of human problems associated with homosexuality.
Unfortunately, most researchers documenting the evolving lives of individuals in
cohort samples have been oblivious to the predictable overrepresentation of
homosexually oriented individuals in the many problems studied, including mental
health issues such as depression and suicide. This was the case, for example,
with a large sample of individuals, now about 27 years of age, that researchers
first studied at the age of 5 to 6 years, the last data intake occurring at the
age of 21 years. It was then reported that gender nonconformity in preschool
("behaviors that are counter to typical gender norms, such as aggressive
behavior in females and dependence in males") was determined to be one of
the "early gender-specific risks for suicidal ideation" (Reinherz
et al., 1995). For boys, this would be an indication that having a
homosexual or bisexual orientation in adulthood may be significantly
correlated to serious problems at some point in one's life, but students of
homosexuality and related problems have been deprived of this low-cost knowledge
because mainstream researchers have remained ignorant of "the homosexuality
factor" in many youth problems. It is therefore recommended that all researchers
carrying out longitudinal studies should be contacted and advised in this
respect because it is doubtful that anyone has been doing such "informed"
advocacy work in mainstream youth problem research.
Special Samples in Studies of Homosexuality
Special population samples have many roles to play in shedding light on various aspects of homosexuality. A population-based cohort of fraternal and identical twins, for example, may be used to explore the possibility of genes being a factor in the genesis of homosexuality given that "same family" environments are being controlled for with fraternal twins and identical twins, and that identical twins have the same genes. Recently, the twin cohort known as the Vietnam Era Twin Registry (age range = 40 to 60 years) was used by Herrell et al. (1999) to investigate the greater risk for lifetime suicidality of homosexually oriented males compared to heterosexual males. At a 95% confidence interval, the unadjusted matched-pair odds ratios results were 2.4 (1.2-4.6) for thoughts about death, 4.4 (1.7-11.6) for wanted to die, 4.1 (2.1-8.2) for suicidal ideation, 6.5 (1.5-28.8) for attempted suicide, and 5.1 (95% CI, 2.4-10.9) for any of the suicidal symptoms. "After adjustment for substance abuse and depressive symptoms (other than suicidality), all of the suicidality measures remain significantly associated with same-gender sexual orientation except for wanting to die (odds ratio, 2.5 [95% CI, 0.7-8.8])" (p. 867).
Study samples may also be of a human group with attributes making it very expensive to use random sampling to obtain the required numbers of individuals needed to produce statistical significance. For example, Bagley and Tremblay (1997) reported that 1% of young adult males were serious suicide attempters, with 5 out of 8 attempters being homosexual or bisexual. It would be almost impossible, however, to say much with reasonable certainty about the results other than concluding that homosexually oriented males are overrepresented in the male youth group engaging in serious suicide attempts. To better understand the situation, a larger sample of homosexually oriented males who attempted suicide would be needed, but it would take a random sample of about 6,000 male youth in Calgary to generate a sample of 40 homosexual and bisexual suicide attempters for analysis. Studying such large samples is expensive and other types of samples, such as the community based sample of 137 gay and bisexual male youth studied by Remafedi et al. (1991), may be used for the statistical analysis of factors significantly associated with suicide attempts. Most study samples of gay, lesbian, and bisexual individuals have been in this category.
Often enough, researcher may also wish to study homosexuality in other population such as schizophrenic males who form about one percent of the male population and are at extremely high risk for committing suicide: about 10 to 20 percent of them will eventually commit suicide, depending on diagnosis. Assuming that homosexually oriented schizophrenic males form a maximum of 10 percent of this population, it would therefore take a population sample of about 5,000 individuals to generate a sample of 5 homosexually oriented schizophrenic males (or maybe 10 if they are overrepresented), and this sampling result would only reveal their representation in the schizophrenic male population.
A common solution to the high cost of using large random samples is, for example, to study various samples of about 100 mostly schizophrenic males in psychiatric male populations to determine their representation, and five such studies reported representation percentages ranging from 14.1 and 22 percent for males who were homosexually active (Susser et al., 1995: 16%; McDermott et al., 1994: 22%; Cournos et al., 1994: 22%; Kalichman et al., 1994: 22%; Lyketsos et al., 1983: 14.1%). The average of these percentages (19%) indicates that the representation of homosexually active individuals in male schizophrenic populations is about twice their representation in the average population given the 9.2 percent estimate reported by Bagley and Tremblay (1998) for currently homosexually active young adult males. One study also reported that none of the homosexually active schizophrenic males perceived themselves to be homosexual (Cournos et al., 1994). The implications are that schizophrenic males acting on their homosexual desires is independent of the "identity" concept so often mentioned in association with modern restricting concept of male homosexuality.
Three of the above cited studies also reported that 10 to 50 percent of homosexually active mostly schizophrenic males had traded sex with males for goods or money (Susser et al., 1995; Cournos et al., 1994; Kalichman et al., 1994), meaning that most of these males may be much like "trade males" of a former age of male homosexuality described at the beginning of this paper. Some of these males, however, may be at risk for sexual assault given that, in one Toronto study of sexually assaulted mostly young adult males visiting a sexual assault center, 35 percent were reported to have cognitive deficits, but a possible link to mental disorders such as schizophrenia or other psychiatric problems was not mentioned (Stermac et al., 1996).
Very little has been written about homosexuality and its effects in the sector of the population deemed to have mental disorders, but the above data indicates overrepresentation, and the similar results were produced from HIV/AIDS related cohort studies of gay and bisexual adult males. Compared to general male population studies, as noted above, gay and bisexual males have high incidences of major depressive disorder (MDD) in the psychiatric history, and they are overrepresented in personality disorders often associated with elevated rates of suicidality.
As a rule, the homosexuality factor in
suicide problem of males with psychiatric diagnoses has been ignored, even
though there are indications that homosexuality is overrepresented in the
suicides of psychiatric patients. One two-year follow-up of 2,753 adults
hospitalized for depression and/or suicidality reported that being bisexual or a
celibate homosexual was one of the 15 variables implicated in suicides (Motto
et al., 1985), and a seven-year follow-up of 500 psychiatric patients
reported that homosexuals accounted for one-third of the suicide deaths.
Interestingly, the authors noted that the study represented the first attempt to
ascertain the sexual orientation of such study subjects (Martin
et al., 1985), and the endeavor has not been repeated possibly die to
indifference.
The role of Grounded Theory and Ethnomethodology Studies in the Research of Male Homosexual Realities.
Studies of the many facets of male homosexuality requires the application of an important rule noted by The Working Group (1995) in the first special issue on "sexual orientation" of Suicide and Life-Threatening Behavior.
Researchers must know the community they are studying (p. 83).
A major problem with the concept of "gay community," however, is its constituents. Who are they? During the period that bisexual people were not supposed to exist, were bisexual individuals a part of "the gay community"? What about schizophrenic males who are homosexually active and may be sexually relating with gay identified males? Homosexual and bisexual males of color have a near double representation in telephone surveys, forming about one-third of homosexual and bisexual identified males, but are they a part of "gay communities" which historically have been white dominated and racist in nature? Is it possible then that the concept of "the gay community" is but a minority subset of the modern world of male homosexuality, as gay identified males also happen to be from a historical perspective?
The problems I have observed gay and bisexual youth manifesting when they venture into "gay communities" are significant and they often continue, sometimes getting worse as often observed with gay male youth with respect to drug use and abuse. As previously noted, the more "feminine" gay males will have significant problems after the venture into "gay communities," but studies are almost nonexistent on the process of integration into "gay communities," and the problems to be encountered by often "at risk" gay and bisexual male youth. Gay communities have also been known for white racism resulting in varied abuses of people of color (Tremble et al., 1989), and there is significant stigma related to "public sex" engaged in by many gay identified males (Tewsbury, 1996). Lying is also common when gay and bisexual males are meeting each other with sexual objectives in mind (de Luze, 1990), and one's class status may also significantly affect one's attachment to gay communities (Chapple et al., 1998).
As demonstrated by de Luze (1990), ethnomethodology studies carried out by researchers participating in the group being studied would greatly improve our knowledge and understanding of what actually exist in the more visible and invisible sectors of gay communities. Some GB male youth, for example, have been reported to be contracting HIV as a way of committing suicide (Johnston, 1995; Tompkins-Rosenblatt, 1997) and, although some gay community individuals have blamed this on society's homophobia (Johnston, 1995, p. 225-6), a recent grounded theory study of gay male youth implicated gay community attributes in the problem (Seal et al., 2000). The study also reported on the likely harmful phenomenon articulated by Kenji Yoshino (2000) in "The epistemic contract of bisexual erasure:" the tacit agreement by the very recent socially constructed gay and heterosexual polarities to invalidate / ignore the existence of bisexual individuals.
It's [the gay community] a very pressuring community. A lot of peer pressure when it comes to being gay or straight. For some strange reason bisexuality isn't really considered sexuality. Bisexuals are seen as gay men who are having trouble with their sexuality. Like it is the first stage of coming out. If someone is really bisexual, people will harass them until they say if they are gay or straight. It's more or less, you know you're gay, get over it (Seal et al., 2000, p. 13).
Recommendations have been made for "participant observation" ethnomethodology studies to be done in gay communities (Weston, 1993; Boulton, 1995), much like the study done by de Luze (1990), but a significant number of gay leaders may not want certain community truths to be known, apparently because it will make gay communities look bad in the eyes of mainstream society. Problems, however, cannot effectively tackled unless implicated realities are acknowledged and addressed.
It is therefore very important to study the lives of homosexually oriented male adolescents and young adults who are at risk for suicide problems - likely to also be present in association with individuals testing HIV-positive (Forstein, 1994; Siegal and Meyer, 1999) - and especially the factors "actually" implicated or "causal" for individuals contemplating the end of their lives, and for the ones who will commit suicide. Our feelings are within our minds, meaning that the "why" questions must be asked, and the answers will likely be subjective in nature, often informing the researcher that there is much more to a decision to kill oneself than significantly correlated items (such as a male being "feminine," abusing drugs and/or alcohol, etc.) often encountered in quantitative studies. For some individuals, manifestation of suicidality may also be a way of working though other life threatening problems as reported in the Siegel and Meyer (1999) qualitative study. A friend wrote the following about "grounded theory" in his 1997 doctoral thesis proposal:
Grounded theory was developed as a method of inductively generating theory from data in order to counter what its creators saw as "the embarrassing gap between theory and empirical research" (Glasser and Strauss, 1967, VII). In their Original work, Glasser and Strauss discovered how categories of meaning related to dying emerged from the study of interviews with medical staff treating terminally ill patients. The concepts that manifested themselves were seen as thus being "grounded" in the data rather than being imposed by theory. Grounded theory has been chosen for the [doctoral thesis] study because the method respects subjective meaning of people's experiences.
The suicide problems of homosexually oriented male adolescents and young adults have generally not been explored by researchers using a "grounded theory" approach, and the method is needed to identify significant factors associated with the suicide problems of homosexually oriented male adolescents before and after they make contact with gay communities. At best, some quantitative studies of at risk individuals contain indication that suicide problems have not ended for studied individuals. The Remafedi et al. (1991) data indicates that about 20 percent (28/137) of studied gay and bisexual male youth were not in the category of "no current suicide intent," and 46 percent (13/28) of these males had attempted suicide. Another 3.6 percent of gay and bisexual male youth (5/137) had a suicide plan, and 60% of them (3/5) had already attempted suicide. Given that suicide is rare for male youth (approximately 1/5,000/year in average population, but the rate would be much higher in gay and bisexual male population), these "at risk" gay and bisexual male youth may be the ones eventually committing suicide. Therefore, improving our understanding of the most "at risk" individuals would require venturing into their minds to discover related perceptions, and a grounded theory approach is recommended to better understand suicide issues from the perspective of the ones having these problems.
Conclusion
The first book on the suicide problems of homosexually oriented individuals, I thought People Like that Killed Themselves, was written by Eric Rofes (1983) who later also became very concerned about the ongoing great abuse of "sissy boys," as he described himself to be in childhood and adolescence (Rofes, 1995). One mother I interviewed in 1996 reported that her 14-year-old son had hung himself in the Calgary Detention Centre in 1995, and that he had an abuse-related "sissy" history dating back to preschool. By the age of 13, however, he changed, becoming a tough delinquent, as Rofes (1995) also reported seeing some sissy boys eventually doing. About two months before his death, his mother had asked him if the nice boy he once would ever return, to which he replied: "Why? To only get beaten up again?"
The second mother interviewed had a same-age son who committed suicide in 1995, and a related Canadian W-5 documentary noted his abuse by others on the basis of his gender nonconformity. The third Calgary mother interviewed had also lost her 17-year-old son to suicide in 1995, but she did not know about his homosexual orientation which had been reported to me by a female friend. His death was also the highlighted case in a feature January 29, 1996 article on youth suicide in Maclean's, Canada's national news magazine. The title of the article, "Killing The Pain: Canada has an alarming rate of teenage suicide - and nobody, including grieving parents, knows why," contained the 'truth' that most people do not know why male youth commit suicide. Maybe, however, this is the predictable outcome when so few have sought to actually know why some adolescent males kill themselves. With respect to Maclean's highlighted case of a male youth suicide, for example, someone knew that "D" was gay, but no one was asking related questions, and I was given the information only because the informant felt I should be told the truth about her friend's death given the nature of my work and concerns.
In addition to the three cases of adolescent male suicide associated with parents who had become part of a SPAN (Suicide Prevention Advocacy Network) group in Calgary, two more parents in the group each had a son who committed suicide. One of the victims was Bobby Steele, a 19-year-old Edmonton male who had committed suicide in 1994. Although some people knew he was gay, such as the publisher of Edmonton's gay magazine and a gay Native American friend, the boy's connection to the gay community was only discovered after a journalist began investigating the case for a major Edmonton Journal story on his death. His father, a Fundamentalist Christian, was also refusing to accept that his son was gay, his attitude being that the "gay" label given to his son was "slander."
From this group of five parent who experienced the suicide of adolescent sons, the two older males were known to be homosexually oriented by some individuals, and the two younger males had a long "sissy" history with related abuses. As for the fifth case, the parents did not volunteer information about their son, and their silence made me suspect that the issues I was addressing were also related to their son. Although this is a small sample, the results are telling, and indicate that the issues addressed in this paper are very much related to adolescent male suicides. Unfortunately, it does not seem that mainstream suicidologists have positioned themselves to uncover the "homosexuality" and/or "sissy boy" factor implicated in adolescent male suicides.
This paper has also presented other factors implicated in elevated rates of suicidality in homosexually oriented male adolescent and young adults. These male are at much greater risk for suicide problems than their heterosexual counterparts for a number of interrelated reasons requiring further study. They are also at the greatest risk for the more serious suicide behaviors, leading to their postulated overrepresentation in suicide statistics. Given the evidence, and my personal experiences in the field as rendered above, I have little doubt that homosexually oriented males account for about two-thirds of male youth deaths from suicide, and the estimate is equal to a little more than half of all youth death from suicide in North America.
This outcome, however, is the likely result of a social construction, the primary one being the transformation of male homosexuality into a rarity as the twentieth century progressed. The resulting modern belief is that homosexual males are so rare that many individuals believe that some rare genetic anomaly affecting no more than one ot two percent males is responsible for homosexual desires. This is unlikely, as evidenced in the historical record related to male homosexual desires, including the potential for associated love responses between males.
Unfortunately, a number of socially constructed forces, including the ones produced by males identifying as "gay," have worked collectively to deny the historical fact that homosexuality is a part of the positive human male potential greatly influenced by one's culture. The price paid for this politically motivated outcome is also extremely high if, in fact, the social construction of male homosexuality into its modern "rare" status is the underlying cause of the majority of increasing male youth deaths from suicide since 1950.
Notes
Note 1: All
binaries have increasingly been questioned as illustrated by Englert (1995)
quoting Robyn Wiegman, a co-editor of the forthcoming book, "Demanding
Discipline: On the Emergence of Gay and Lesbian Studies": "Wiegman points out.
The current concepts of heterosexuality / homosexuality, black / white, male /
female, are artificial binaries: 'The more you think about this, the more you
realize that these binaries cannot hold up. The actual multiplicity and variety
of humans on the planet is absolutely non-binary, yet we're so wed to the binary
concept and it scares us to think otherwise..." Challenges to the binary
concepts have been embodied in titles of books such as "Third Sex, Third Gender:
Beyond sexual dimorphism in culture and history" (Herdt, 1994)
and
Beyond Gay or Straight: Understanding sexual orientation (Clausen,
1996). In a study of working class males from the Australian city of
Nullangardie, Dowsett (1994) not only places current
concepts of sexual orientation in question on the basis of the evidence, but he
also states "the usefulness of the now-classical concepts of sexual identity and
gender identity will be questioned as being too narrow and locked into
questionable binary oppositions."
Note 2: Tremblay (1998) summarized the status of bisexuality in the research world by stating that, even though Kinsey's 1948 research indicated significant bisexuality in males, it was only as the result of AIDS-related research that the concept began to surface again in discourses by researchers. "Essentially, sexual orientation has been presented as a homosexual / heterosexual dichotomy, with nothing in between. For too long bisexuality has been perceived as a transition and, by definition, unstable, linked to adolescence, to the absence of a female partner (as in the case of prisoners), or to economic reasons (as with prostitutes)." (Translated by author.) Dorais (1994) noted the same fact which was also reflected in a recent study of papers published in 17 family therapy journals from 1975 to 1995. Clark et al. (1997) reported that only .006% of the articles (n = 77) focused on homosexuality issues, and that "only two [of these] studies included bisexuals, indicating a dearth of knowledge in this area" (p. 248). Also indicated, however, is the complete absence of "bisexuality" from the consciousness of family therapists, as I witnessed in 1994 at a meeting of professionals concerned about homosexually oriented youth. Calgary's leading expert on "homosexual orientation" issues (a family therapist of high stature who headed the list for related referrals by my family doctor) reported that, in his practice, bisexuality was responded to as a nonexistent entity. One's clients were to be either homosexual or heterosexual and 'therapy' would proceed accordingly so that the results, even if some clients were being harmed, would not conflict with the therapist's beliefs about the binary nature of sexual orientation.
In gay and lesbian communities, the general response to bisexual individuals has also been to negate their existence because they were perceived to challenge the belief that only heterosexual and homosexual people existed. Many bisexual individuals have reported on their abuses in gay and lesbian communities. Tisdale (1998) writes: "Many gay activists see any talk of bisexuality as diluting the coherence of the community, particularly damaging in a time of attack... Others simply don't believe in bisexuality, seeing through the lens of their own difficult coming-out experience... Bisexuals hear the same things from straights and gays, friends, lovers and perfect strangers: You can't be both. You can't be neither. You just haven't faced the truth. You're secretly wishing for A or B. Insert gay, insert straight, and it comes out the same - something essential is denied." A similar situation is described by Button (1998): "As a bisexual woman... I have been called a fence-sitter, disease-carrier, AC/DC, confused, etc. by gay and lesbian communities."
In an interview, Kenji Yoshino, the author of "The Epistemic Contract of Bisexual Erasure" published in the Standford Law Review (Yoshino, 2000), summed up the situation for bisexual individuals: "Advocate: It's a conspiracy. Yoshino: Yeah. My theory is that both gays and straights have agreed that, no matter what else they disagree on - they disagree on a lot - they'll both agree about this one thing, which is that bisexuals don't exist. Because they have different but overlapping interests in erasure. If the realm of bisexual possibility exists, it becomes impossible to actually prove that you're straight or you're gay. If you're straight in a world where bisexuality doesn't exist, then you can prove you're straight simply by adducing cross-sex desire: like, "I have a wife, I have a girlfriend" - if you're a man - kind of thing. Right? Whereas, once you introduce a bisexual possibility, the fact that you have cross-sex desire does not [prove] that you don't have same-sex desire. Given that same-sex desire is stigmatized, people who want to identify as straight are going to have a lot invested in making sure that they can prove that they're straight. Because otherwise they'll lose heterosexual privilege... One of the things that both straights and gays, according to their own accounts, feel [is] threatening about bisexuals is that bisexuals are seen to be gender-blind" (Bass, 1999). The elimination of bisexuality began in the professional with individuals such as Sandor Rado (1940) who was quoted in the following way: "..biologically speaking, 'there is no such thing as bisexuality either in man or in any other either vertebrate.' except for developmental disturbances that are clearly recognizable as 'inconsistencies of sex differentiation' (p. 464)" (Quoted by Marmor, 1981, p. 14.) Many in gay communities and professional worlds bought into a generalized view of this ideology (written to invalidate Freud's belief about innate human bisexuality), to the point that bisexuality was widely given a non-existent status by the 1980s and 1990s. As a result, there were great abuses by gay and lesbian identified individual (and professionals with similar beliefs, including therapists) of individuals daring to assert their bisexual orientation.
Individuals who are well versed on issues related to sexual orientation rendered by the Kinsey (1948) 7-point "homosexual to heterosexual" scales for behavior and fantasy, Klein's sexual orientation scale or grid (Weinrich et al., 1993; Keppel and Hamilton, 1998), and especially contemporary and historical cross-cultural anthropological knowledge of human sexualities (Carrier, 1981; Murray et al., 1992: Werner, 1998; Murray and Roscoe, 1998; Halperin, 2000, may reach the conclusion arrived at by Peter Voeller (1997) as the result of attending comprehensive lectures on sexual orientation given by Lois McDermott, Department of Psychology, University of Washington. "General thoughts taken away from the lectures: The idea of sexualities and the fluidity of human sexual experience, shown by her figure of a total of as many as 400 homosexualities, heterosexualities, and bisexualities. This theory has unfolded in order to capture not only the well-established and clear-cut distinctions like gay and straight, but also newer distinctions, like transsexuality and transvestism, in order to distinguish more of the variety within the broader rubric of sexual orientation."
Note 3: Kinsey et al. (1948) reported that 37 percent of males had experienced at least one orgasm while relating sexually with another male between the onset of adolescence and old age. Given that Kinsey's sample also included young males, and that some of these individuals reporting no homosexual experiences when interviewed may have experienced same-gender sexual experiences later, the life time incidence would be higher than that reported for the sample. In addition, another 13 percent of males with no homosexual experience did report having related desires, probably not being incidental. Given the modern idea that "sexual orientation" is apparently not to be based on "behavior," but on desire (which may not be acted on), these males would certainly not be in the exclusive homosexuality category. Twenty-five percent (25%) of males were reported to "have more than incidental experiences or reactions (i.e., rates 2-6) for at least three years between the ages of 16 and 55 (pp. 650-1)".
Kinsey et al. (1948) also reported that "there is much more homosexual activity among males of lower educational level [forming the working classes] than there is of males of the college level [generally forming the middle classes]," the differences being in the order of "200 to 500 per cent." A lesser difference - "not more than 50 to 150 per cent, and sometimes they are not even 10% - occurred between religiously active and religiously inactive groups" (pp. 482-3). Interestingly, the highest reported incidence of homosexual outlet for any group (59.4%, age: 16 to 20) was for single males with an educational level of grades 9-12 (the predominant education level of males in the neighborhood in which I grew up), who were also inactive Catholics as many males in my community were by that age, or soon became.
Given the above stated incidence of 37% for homosexual male activity to orgasm, and 13% for reporting related desires not yet acted upon at the time of interview, the fact that some would have eventually acted on their desires, and the significant class effect (200% to 500% difference) with respect to males having engaged in homosexual activity to orgasm, it could be concluded that more than 50 percent of the working-class males who formed the majority male population in the first half of the 20th century in the United States were manifesting either homosexual desires or the ability to have orgasms when relating sexually with another male. My own experience (Bagley, 1997) indicates that almost all males throughout adolescence may also manifest their potential to enjoy relating sexually with other males, and also seek out such encounters, to a degree reaching the 80 to 90 percent level, much like the situation which had existed in Ancient Greece. However, age difference, or sex role difference (i.e., being dominant or passive in accordance to socially prescribed sex roles), did not apply in my community Therefore significant behavioral variation may be expected in populations of males where high rates of homosexual activity has been reported.
An example of a form of male homosexuality quite alien to my adolescent male collective was given in the Dowsett (1994) study. He reported that in the Australian working-class city of Nullangardie where male homosexuality was exceptionally common, "men in the study reported that their school friends told each other of the places to get sex with other boys and older men." This indicates that male homosexuality is related to sex roles, such as only being dominant and passive, and an important question came to mind as I read this. Discourses by adolescent males may not reflect, in some significant ways, what actually occurs in more private spaces. Therefore, in an environment where adolescent males casually and positively discuss the places where one can have sex with other males, it is possible that some or many of these boys may be also relating sexually with each other, and sexual activity may not be in the apparently prescribed active-passive male-female heteronormative manner. Dowsett (1994) does not seem to have explored this possible reality for male adolescents in Nullangardie.
Note 4: At the age of 11 or 12, a best friend and I were discussing whether or not what we were doing sexually was a sin, the thought being that our sexual activities were most natural even if it was to be private in nature. By then, we had been told that sex with females was sinful (adultery, if one is not married), but no one talked about sex between males. Our first conclusion was that a male having sex with a female was sinful because the two individuals were different. In our situation, however, because we were the same, it was probably not a sin. I nonetheless decided to check this out with priests in confession, without directly asking, but by incorporating my homosexual activities in the list of sins. Reflecting on this, I still find it most amazing that not one priest, out of many to whom I confessed my sins, ever mentioned anything specific to me about this sin, and the penance I received after I began adding the homosexual sins to the list were the same as it had been before. The conclusion was therefore that this was a sin, but nothing special. Maybe something not worse than telling a lie.
Note 5: In the past few years I have encountered two reports, both from England, of adolescent males who had joined navies only to then become the property of a male who sold their sexual services to others on the ship. One individual had joined the Royal Navy at the age of 16 in the early 1960s, and the other had become part of the merchant marine in the 1940s, both eventually obtaining their PhDs and becoming researchers. Given that the availability of these boys was widely known on the ship and that they were used extensively both by their 'owners' and others, these cases indicate that navies were very much in need of the infamous "cabin boy" so often spoken of "sexually' in legends. This phenomenon is also remarkably similar to one aspect of the male homosexuality reported to have been the rule in 19th century male prisons (Ellis, 1906) and also by individuals reporting on the North American prison situation in the 1960s and 1970s (Scacco, 1982; Donaldson, 1993; Caron 1979). There are some indications, however, that the extent of homosexuality in North American prisons has lessened in the last 20 years, but the situation seems to have continued in Australia given that a recent study reported that about 25% of male youth entering prisons are raped by other males apparently in need of male sexual services, with or without the consent of the targeted desired male (Murphey, 1998). The Reiss (1961) study reports that about 60 percent of American "career delinquents" were also involved in "trade" situation with homosexual-identified males when they were not in prison, most often for money, but that they also participated in such activity for free, the motive being the enjoyment of such activities. The title of the study, The social integration of peers and queers, implies a social construction remarkably similar to the situation reported in the Nilsson (1998) study which could have been titled "The social integration of real men and men who were so."
Note 6: Garofalo et al. (1999) reported that GBN males (gay/bisexual identified, and the ones not sure of their sexual orientation) were 6.5 times more likely than heterosexual males to report a suicide attempt in the past 12 months, but it was apparently not deemed important to report the percentage of suicide attempters in each category. Given, however, that males had a suicide attempt incidence (for a 12-month period) of 6.4% and using an estimate of about 4.7% for GBN males (3.8% GB males + 0.9% "not sure") in calculations, the relative incidence of suicide attempters would be 33% versus 5.1% for GBN males compared to heterosexual males. On the basis of this estimate, another estimate is also possible. About one quarter - 24.3% - of male suicide attempters are in the GBN category. Therefore, 4.7% of the students in the GBN category account for about 25% of the male suicide attempt problem.
Note 7: The suicidality data intake methodology used by Bagley and Tremblay (1997) is known in the field of American suicidology. In fact, Moscicki (1989) deemed Bagley & Ramsay's 1985 distinction between "self-harm" and "suicide attempt" to be "very important," and she reported on the methodology. "Respondents were asked in a semi structured interview about sociodemographic characteristics, childhood history, social ties, religiosity, stress, health, 'suicidal behaviors,' and 'suicidal actions': 1. Have you ever felt that life was not worth living? 2. Have you wished that you were dead - for instance, that you could go to sleep and not wake up? 3. Have you ever thought of taking your life, even if you would not really do it? 4. Have you ever reached the point where you seriously considered taking your own life and perhaps made plans how you would go about doing it? 5. Have you ever deliberately harmed yourself, but in a way that stopped short of a real intent to take your life? 6. Have you ever made an intentional attempt to take your life?" The six items are cited from the Appendix in Ramsay and Bagley (1985, p. 165), and the correlates of suicidal behavior were published in the same year by Bagley and Ramsay (1985).
To date, most American suicidality research has ignored the last two distinctions noted by Moscicki (1989) to be very important, and a study that Moscicki's research team published in the same year had also ignored this distinction (Moscicki et al. 1989). Under the heading of "limitations" for their study, the following caveat was written. "'Suicide attempt' could thus have been interpreted by the respondent as an act of deliberate self-harm without the intention of dying, a genuine (and failed) attempt to end one's life, or as something else (perhaps an 'accident' had been explained to them by a physician that had seen it as an unconscious suicide attempt). Suicide ideation, similarly, may mean different things to different people (p. 122)." This serious nomenclature problem was noted by O'Carroll et. al. (1996), with recommendation being made. After reviewing these recommendations, Bagley and Ramsay (1997) stated: "Our definition of suicidality generally accord with those proposed by O'Carroll et al. (1996)" (p. 7).
Note 8: Using the 2 X 2 Table located at - http://home.clara.net/sisa/twoby2.htm and the following data from the Bagley and Tremblay (1997) study - 5 attempters and 77 GB non-attempters (homosexual or bisexual) versus 3 attempters and 665 heterosexual non-attempters, - produces an OR (Odds Ratio for attempting suicide) = 14.4 (95% CI, 3.4-61.4). The OR for "Self-Harm" (13 GB males reporting self-harm, 69 not reporting self-harm / 37 heterosexual males reporting self-harm and 631 not reporting self harm; - produces an OR (Odds Ratio for self-harm) = 3.2 (95% CI, 1.6 - 6.3). The related Chi Square significance is 22.1, p < .0000 and 12.5, p = .0004, respectively.
The "suicide attempt" OR for the Bagley and Tremblay (1997) study of homosexual and bisexual males versus heterosexual males ranging in age from 18 to 27 years (Mean = 22.7 years) - is similar to the OR calculated for the Bell and Weinberg (1978) data for male to the age of 21: 14.9 (95% CI, 3.6-61.6) - Predominantly homosexual males versus predominantly heterosexual males: 55 suicide-attempters / 520 nonattempters versus 2 suicide attempters / 282 nonattempters. These ORs are also similar to the estimated ORs calculated from the data given by Cochran and Mays (2000) for males (age range = 17 to 29 years) reporting having only female sex partner(s), or males reporting not having had any male sex partners, versus males reporting having had a least one lifetime same-sex partner. Respectively, the ORs are 12.5 (95% CI, 6.4-24.2) and 13.8 (95% CI, 7.1-26.8). These Odds Ratios were calculated using the 2 X 2 Table located at - http://home.clara.net/sisa/twoby2.htm and the following estimated data:
Odds Ratio Calculation for males reporting lifetime male sex partner(s) compared to males reporting only female sex partner(s): 15 / 32 (attempters / nonattempters) versus 60 / 1595 (attempters / nonattempters), - 95% CI, Odds Ratio: 6.41<12.46<24.24.
Odds Ratio Calculation for males reporting lifetime male sex partner(s) and males reporting only female sex partner(s) plus males reporting a celibate status: 15 / 32 (attempters / nonattempters) versus 61 [60 + 1] / 1796 [1595 + 201] - 95% CI, OR: 7.10<13.8<26.82.
Information related to all above estimated OR values is available at - http://www.virtualcity.com/youthsuicide/gbsuicide1.htm .
Note 9: For a sample of 28 male and 20 female homosexual (88%) and bisexual (12%) individuals, Hammelman (1993) reported that 64% of the suicide attempters had identified their homosexuality to have been a part (35%) or most (29%) of the problem linked to their suicide attempt. Information was not solicited, however, to permit a reporting on the possible relationship of some suicide attempts to homosexual relationship problems.
Note 10: Drug use and abuse by homosexually oriented adolescents in school compared to heterosexually oriented adolescents.
Garofalo et al. (1998): Results for grades 9 to 12 Massachusetts' students (1995 sample), comparing 2.5 percent of gay, lesbian, and bisexual identified students with heterosexually identified students in grades 9 to 12:
1. Cocaine use before the age of 13 (17.3% vs 1.2%: 14.4 times).
2. Cocaine use in last 30 days (25.3% vs 2.7%: 9.4 times).
3. Cocaine use in lifetime (33% vs 6.9%; 4.8 times).
4. Crack or freebase use in lifetime (35.3% vs 3.5%: 8.9 times).
5. Shared needles for illicit drug use in lifetime (15.5% vs 1.1%: 14.1 times).
6. Anabolic steroids use in lifetime (25% vs 3.9%: 8.4 times).
7. Injected illegal drugs in lifetime (22.2% vs 2.3%: 9.6 times).
Levine and Beeler (1997)
[Related published paper: Faulkner et al. (1998)]:
Results for grades 9 to 12 Massachusetts' students (1993 sample), comparing 3.7
percent of students who reported having been homosexually active to students who
had been only heterosexually active:
1. Involved in episodic heavy drinking (15.0%% vs. 3.8%: 4 times).
2. Currently consuming alcohol every day (10.9% vs 1.2%: 8.7 times).
3. Used cocaine at least once (19.2% vs 3.2%: 6.0 times).
4. Used cocaine 10 or more times (13.3 vs .7%: 19 times).
5. Used illegal drugs other than alcohol, marijuana, or cocaine (17.8% vs 3.5%: 5.1 times).
6. Injected illegal drug (20.8% vs 3.1%; 6.7 times).
Smith et al (1999): Six percent of a sample of 3,387 Australian students in grades 10 to 12 reported same-gender sexual attraction. "Being attracted to members of the same-sex was associated with more frequent binge drinking among boys and girls, and a three- to four-fold increase in the likelihood of reporting injecting drug use both over the lifetime and within the previous 12 months" (p. 643).
Note 11: Using the 2 X 2 Table located at - http://home.clara.net/sisa/twoby2.htm - and the following data from the Remafedi et al. (1991) study 38 gay and bisexual male suicide attempters classified as feminine, androgynous, and undifferentiated, and 71 nonattempters in the same categories versus 3 "masculine" attempters and 25 "masculine" gay and bisexual male non-attempters - produces an OR (Odds Ratio for attempting suicide) = 4.5 (95% CI, 1.3 - 15.7). Chi Square: 6.2, p = .013. The Risk Ratio = 3.2 (95% CI, 1.1 - 9.8).
Note 12: French texts by de Luze (1990) translated by author:
La vérité est souvent rebutante. La plupart des homosexuels que j'ai rencontrés ne tiennent pas à la connaître (malgré leurs professions de foi contraire)... L'usage si fréquent du mensonge chez les dragueurs homosexuels pose parfois des problèmes. Par exemple dans les cas où, succédant au simple plaisir, s'installe la passion. Peut-on envisager une liaison? Sur quelle base? Où va-t-on ainsi à l'aveuglette? En fait, quand on a affaire à un menteur enraciné, il n'y a guère de moyen rationnel pour détecter où finit le mensonge et où commence la vérité (de Luze, 1990: Conclusion).
Les muscles de Guy sont un effort désespéré pour faire croire qu'il est un mec sûr de lui, résolu, moralement solide, alors qu'en fait c'est un garçon timide, complexé, maladivement nerveux, perpétuellement anxieux comme je m'en rends compte au fur et à mesure que la soirée s'avance et que, l'alcool lui donnant un peu d'assurance, un maniement plus aisée de la parole, il finit par se confier et nous révéler qu'il est constamment dépressif et a déjà fait trois tentatives de suicide (de Luze, 1990: Mensonge du Paraître: Muscles).
Note 13: A response to "gay stereotype" issues mentioned in the Final Report of the 'Here for Life" Youth Sexuality Project was sent to Graham Brown, the contact person for the Final Report. The exchange of information resulted in a revised section addressing a number of related issues. Permission was requested to quote from the emails by sending a draft of the section for approval and related comments. A final version was then sent, and permission to quote was granted. A related comment by Graham Brown: "While I may not totally agree with all your conclusions, I agree with the general thrust, and anyway it is not for me to necessarily agree or not, but for you to put forward your thoughts and arguments, and I am happy to contribute to that." He also volunteered to have his email given - [email protected] - should anyone reading this section of the paper wish to have someone with whom some important multi-dimensional issues relating to the organization of sexual minority youth groups may be discussed, including the development of potential problems, gay stereotypes, etc.. Graham Brown's Address: WA AIDS Council, PO Box 1510, West Perth, WA 6872, Australia.
Note 14: The issue of adolescent and young adult males being raped after they have become integrated in gay communities is generally ignored. Often enough sexual assaults occur after meeting gay or bisexual individuals in a club or a community group, and then finding themselves in a more private location such as a home or an apartment. In such a situation they may discover their loss of right to not have sex with the individual, and a sexual assault results. As a rule, the raped individuals I have interviewed were more "feminine" in nature, and physically not imposing, although this was not always the case. One 17-year-old Calgary male youth of decent physical stature reported that his size became irrelevant mostly because the two gay males (about 40 years of age) he had met at a gay club participated in the rape after he had accepted an invitation to their home. All raped individuals had also not reported the rape to authorities mostly because they did not want their "homosexuality" to be public knowledge, and this fact essentially gives gay and bisexual rapists an open license to rape. The raped individuals had also not sought counseling related to the rape.
Some raped gay and bisexual males, however, do seek help, and a group of these males in Toronto was reported on by Lana Stermac et al. (1996). They noted: "...that the majority of [mostly young adult male] victims [of sexual assault or rape] are gay or bisexual and are at least acquainted with their assailants [who are also mostly homosexual or bisexual] - have been supported by other recent investigations of sexual assault of males and studies of sexual coercion in dating relationships of adult males" (p. 61). The mental health and suicidality effects of gay community based sexual assault and rape on homosexually oriented male youth, especially adolescents, remain to be studied. A contributing factor to this problem may be related to an observation made about many gay males, one of these being the responses of about 10 gay males present at Calgary Gay Lines one evening. They were most opposed to the idea of meeting a gay male, ending up in a private space, and then having the desired male not want to relate sexually with them. My response to such attitudes was to highlight the fact that many heterosexual males have used the same ideology to justify their date raping activities with females.
Remafedi et al. (1991) reported high rates of sexual abuse for gay and bisexual male youth (39%), but also noted that the reported sexual abuse generally postdated sexual identification as gay or bisexual. The unspoken implication is that the sexual abuse likely occurred after they made themselves available for sexual experiences often occurring via making contact with some gay community attribute such as the "public sex" arena, as most of the first sexual experiences occurred for the teenage gay males studied by Uribe and Harbeck (1992). Sexual assault and rape after adolescent males have made contact with gay communities, however, remain hidden in all studies reporting such experiences, often assumed to be "child sexual abuse" having occurred before the individual made contact with gay communities. This assumption may be incorrect. In a 1989 study of 46 male youth prostitutes (average age of 16.2 years, 70% GB males), 72% of the gay and bisexual males had been sexual abused compared to 43% of heterosexual males, 43% of gay and bisexual males had been raped compared to 21% of heterosexual males, and 85% of the rapes had not been related to their street life (Boyer, 1989).
By the year 2000, the research silence on sexual abuse and rapes of young gay and bisexual males in gay communities had been broken. From a qualitative study of 30 gay-identified male youth ranging in age from 18 to 24, Mutchler (2000) reported that "more than half (18 out of 30) of the young men in this study told of feeling pressured or forced into having sex that they did not completely want. Nine of these individuals were raped by boyfriends, family members, or other men" (p. 31), and four of the nine "were raped by men other than their boyfriends" some at a very young age, with the majority (5/9) being rapes by boyfriends (p. 32). Mutchler noted, however, that "the line between being used and being raped is fussy under [some] situation" (p. 32). For example, he reported on a youth meeting an older man (previously unknown to the youth) and ending up in a situation where the sex (including being subjected to unwanted unprotected anal sex) was experienced. The youth reported his feelings:
I was afraid he would get mad at me or something. I don't know. It was pretty stupid. I don't feel good about it; it's a pretty bad way of treating a person, but it's pretty common in the gay world. When I went to [the gay bar], it sort of felt like the people were circling me like hawks (p. 31).
Mutchler noted that "stories like [the one above], with slight variations, [were] repeated by 11 of my 30 respondents" (p. 31).
Note 15: "A
New Zealand study being conducted by researchers at the Dunedin School of
Medicine (for information please contact Shyamala Nada-Raja - Email:
[email protected]) will determine the association between sexual
orientation (based on a measure of sexual attraction) and a range of behaviours
indicative of deliberate self-harm (suicidal, non-suicidal intent). The study is
based on the Dunedin Multidisciplinary Health and Development Study (DMHDS). The
findings are expected to complement those reported by
Fergusson and colleagues (1999) in the Archives of
General Psychiatry." (Cited from a March 21, 2000 email from Shyamala Nada-Raja
written in response to a request made by Pierre Tremblay for information to be
included in this note.)
Bibliography
American Psychological Association (1999). Answers to Your Questions
About Sexual Orientation and Homosexuality: Definition of sexual orientation.
Internet Page: -
http://helping.apa.org/daily/answers.html
Atkinson J, Grant
I, Kennedy C, Richman D, Spector S, and McCutchan A (1988).
Prevalence of psychiatric disorders among men infected with immunodeficiency
virus. Archives of General Psychiatry, 45, 859-64.
Bagley, Chris (1997).
Policies for gay and lesbian youth. In Chris Bagley.
Children. Sex and Social Policy: humanistic solutions for problems of
child sexual abuse, 176-180. Aldershot, England: Avery. Relevant
Section, pp. 183-5 is available (with additional information) on the Internet: -
http://www.virtualcity.com/youthsuicide/adams.htm .
Bagley, Chris,
Bolitho F, and Bertrand L (1995). Mental health profiles, suicidal
behavior, and community sexual assault in 2,112 Canadian adolescents.
Crisis, 16, 126-31.
Bagley, Chris, and
Ramsay, Richard (1997). Suicidal Behavior in Adolescents and Adults.
Aldershot, England: Ashgate.
Bagley Chris, and
Ramsay, Richard (1985). Psychosocial correlates of suicidal behaviors in
an urban population. Crisis, 6(2), 63-77.
Bagley, Chris, and
Tremblay, Pierre (1998). On the prevalence of
homosexuality and bisexuality in a random community survey of 750 men aged 18 to
27. The Journal of Homosexuality, 36(2), 1-18. Internet Availability: -
http://www.virtualcity.com/youthsuicide/homodemo.htm .
Bagley, Chris, and
Tremblay, Pierre (1997a). Suicidality problems of gay and bisexual males:
Evidence from a random community survey of 750 men aged 18 to 27. In
Chris Bagley and Richard Ramsay, Eds.. Suicidal Behavior in Adolescents
and Adults, 177-193 Aldershot, England: Ashgate.
Internet Availability: -
http://www.virtualcity.com/youthsuicide/suicide.htm .
Bagley, Chris, and
Tremblay, Pierre (1997). Suicidal behaviors in homosexual and bisexual
males. Crisis, 18(1), 24-34. Internet Availability
(Alternate version of the paper): -
http://www.virtualcity.com/youthsuicide/suicide.htm .
Bagley, Chris,
Wood M, and Young L (1994). Victim to abuser: mental health and
behavioral sequels of child sexual abuse in survey of young adult males.
Child Abuse & Neglect, 1994; 18(8): 683-697.
Bailey, J Michael
(2000). J. Michael Bailey... recent research activities. Internet
Page: -
http://www.psych.nwu.edu/psych/people/faculty/bailey/research.html
Bailey, J Michael
(1999). Homosexuality and mental illness. Archives of General
Psychiatry, 56(10), 883-4. Internet Availability: -
http://archpsyc.ama-assn.org/issues/v56n10/rfull/ycm9269.html .
Bailey, J Michael,
Kim P, Hills A, and Linsenmeier J (1997). Butch, femme, or
straight-acting? Partner preferences of gay men and lesbians. Journal of
Personality and Social Psychology, 73, 960-973.
Bass, Carole (1999).
Both Ends Against the Middle: How gays and straights make bisexuals invisible.
Hartford Advocate, June 17. (Interview with Kenji Yoshino (2000),
author of "The Epistemic Contract of Bisexual Erasure" to be published in
the Standford Law Review.) Internet Page: -
http://www.hartfordadvocate.com/articles/biout2.html .
Bayer, Ronald (1981).
Homosexuality and American Psychiatry: The politics of diagnosis. New York:
Basic Books.
Bell, Alan, and
Weinberg, Martin (1978). Homosexualities: A Study of Diversity Among
Men and Women. New York: Simon & Shuster.
Bell, Alan, Weinberg
M, and Hammersmith S (1981). Sexual Preference: Its Development in Men
and Women. Bloomington, Indiana: Indiana University Press.
Bell, Alan, Weinberg
M, and Hammersmith S (1981). Sexual Preference: Statistical Appendix.
Bloomington, Indiana: Indiana University Press.
Bem, Daryl (1996).
Exotic becomes erotic: a developmental theory of sexual orientation.
Psychological Review, 103(2), 320-335. Internet Availability: -
http://comp9.psych.cornell.edu/dbem/ebe_theory.html - Related publications:
-
http://comp9.psych.cornell.edu/dbem/online_pubs.html
Bem S (1974).
The measurement of psychological androgyny. Journal of Consulting and
Clinical Psychology, 42, 155-162.
Billings, Paul
(1993). Genetic discrimination and behavioral genetics: The analysis of
sexual orientation. In Intractable Neurological Disorders in
Human Genome Research and Society. Proceedings of the Third International
Bioethics Seminar in Fukui, 19-21 November, 1993, 35-39. Internet
Availability:
http://www.biol.tsukuba.ac.jp/~macer/IND/INDPB.html
Boney, Bradley (1996).
The Lavender Brick Road: Paul Bonin-Rodriguez and the Sissy Bo(d)y. Theatre
Journal, 48(1), 35-57. Internet: -
http://muse.jhu.edu/demo/tj/48.1boney.html
Boulton, Ralph
(1995). Rethinking Anthropology: The study of AIDS. In: Han ten
Brummelhuis and Gilbert Herdt, Eds. Culture and Sexual Risk:
Anthropological perspective on AIDS. Amsterdam: Gordon and Breach
Publishers, 285-313.
Boyer, Debra. (1989).
Male prostitution and homosexual identity . In Gilbert Herdt, Ed.
Gay and Lesbian Youth. pp. 151-184. New York: Harrington Park Press.
Also published in the Journal of Homosexuality, 17(1-4), 1989.
Brady S, and Busse W
(1994). The Gay Identity Questionnaire: a brief measure of homosexual
identity formation. Journal of homosexuality, 26(4), 1-22.
Brent David (1995).
Risk factors for adolescent suicide and suicidal behavior: mental and
substance abuse disorders, family environmental factors, and life stresses.
Suicide and Life-Threatening Behavior, 25(suppl), 52-63.
Brighton Ourstory
Project (1992). Daring Hearts: Lesbian and gay lives of the 50s and
60s. Brighton, England: Queenspark Books.
Brown, Graham (2000).
'Here for Life" Youth Sexuality Project: Contact Person. Personal
opinion expressed in three emails to Pierre Tremblay, March, 2000. Permission to
quote granted. Email: [email protected] . Address: WA AIDS Council, PO Box
1510, West Perth WA 6872, Australia. Additional Information:
Note 13.
Button, Heather
(1998). Being bi in a binary world. Internet Page: -
http://www.youthresource.com/women/archives/9808biphobia.html .
Bux D (1996).
The epidemiology of problem drinking in gay men and lesbians: a critical review.
Clinical Psychology Review, 16(4), 277-98.
Caballo-Dieguez A,
and Dolezal C (1995). Association between history of childhood sexual
abuse and adult HIV-risk sexual behavior in Puerto Rican men who have sex with
men. Child Abuse & Neglect, 19(4), 595-605.
Cantarella, Eva
(1992). Bisexuality in the Ancient World. (Trans. Cormac Ó
Cuilleanáin). New Haven, Connecticut: Yale University Press. Scholia Reviews ns
5 (1996) 1 by Eva Stehle: -
http://www.classics.und.ac.za/reviews/96-1cant.html - Scholia Reviews Home
Page:
http://www.classics.und.ac.za/reviews/default.htm .
Carbery G (1992).
Some Melbourne beats: A "map" of the subculture from the 1930s to the 1950s.
In R Aldrich and G Wotherspoon, Eds. Gay Perspectives: Essays in
Australian Gay Culture. Sidney, Australia: Department of Economic
History, University of Sidney.
Caron, Roger (1979).
GO BOY! Ontario, Canada:
Nelson & Sons.
Carpenter, Edward
(1917). IOLÄUS: An Anthology of Friendship. New York: Mitchell
Kennerley. First published in 1909. Internet Availability:
http://www.fordham.edu/halsall/pwh/iolaus.html .
Carrier J (1981).
Homosexual behavior in cross-cultural perspective. In Judd Marmor, Ed.
Homosexual Behavior: A Modern Reappraisal, 100-122. New York; Basic Books.
CDC (1999): Centers
for Disease Control, Division of Adolescent and School Health (DASH).
Assessing Health Risk Behaviors Among Young People. Internet Page: -
http://www.cdc.gov/nccdphp/dash/yrbs/yrbsaag.htm .
CDC (1999a): Centers
for Disease Control, Division of Adolescent and School Health (DASH).
1999 Youth Risk Behavior Survey. Internet Page: -
http://www.cdc.gov/nccdphp/dash/yrbs/survey99.htm .
CDC (1994).
Programs for the Prevention of Suicide Among Adolescents and Young Adults.
MMWR 43(RR-6), 1-7. Internet:
http://wonder.cdc.gov/wonder/prevguid/m0031525/m0031525.asp
Chamberlain,
Claudine (1999). Where Did the Gay Gene Go? Study Finds No Evidence of
Homosexuality in DNA. ABC News, April 22. Internet:
http://abcnews.go.com/sections/living/DailyNews/gaygene990422.html
Chapple M, Kippax
S, and Smith G (1998). "Semi-straight sort of sex": Class and gay
community attachment explored within the framework of older homosexually active
men. Journal of Homosexuality, 35(2), 65-83.
Chauncey, George
(1994). Gay New York: Gender, Urban Culture and the Making of the Gay
Male World, 1890-1940. New York: Basic Books. Book Reviews: -
http://www.usc.edu/Library/oneigla/onepress/reviews/gayny.html -
http://spanky.osc.cuny.edu/~ashp/GayNY.html -
http://www.majbill.vt.edu/students/history5124/Neely.html -
http://www.clas.ufl.edu/users/brundage/20thcentury_grad_course/Chauncey_review.html
Chauncey, George
(1985). Christian Brotherhood or sexual perversion? Homosexual identities
and the construction of sexual boundaries in the World War One era. Journal
of Social History, 19, 189-212.
Clark, Wanda, and
Seovich, Julianne (1997). Twenty years and still in the dark? Content
analysis of articles pertaining to gay, lesbian, and bisexual issues in marriage
and family therapy journals. Journal of Marital and Family Therapy, 23(3),
239-53.
Clacher, Iain
(1997). Silence is where the hate grows: silence = death. Campaign
Australia Magazine. Internet Availability: -
http://www.youth.org/loco/PERSONProject/Alerts/International/suicide3.html .
Clausen, Jan (1996).
Beyond Gay or Straight: Understanding sexual orientation. Philadelphia:
Chelsea House Publishers.
Clayton, Gabi
(1997-2000). Portrait of a Son's Suicide: Bill's Story. Internet
Page: -
http://members.tripod.com/~claytoly/Bills_Story.html - Home Page:
http://members.tripod.com/~claytoly/
Cochran, Susan, and Mays, Vickie (2000). Lifetime prevalence of suicide
symptoms and affective disorders among men reporting same-sex sexual partners:
results from NHANES III. American Journal of Public Health, 90(4), 573-78.
Collins, Chris
(1997). Dangerous Inhibitions: How America Is Letting AIDS Become an
Epidemic of the Young. UCSF AIDS Research Institute (ARI) and The Center for
AIDS Prevention Studies (CAPS). San Francisco: University of California.
Internet:
http://www.caps.ucsf.edu/publications/adolmono.html or
http://www.aids.harvard.edu/lead_initiatives/marketing_health/dangerous.html
Cournos F, Guido J,
Coomaraswamy S, Meyer-Bahlburg H, Nat R, Sugden R, and Horwath E (1994).
Sexual activity and risk of HIV infection among patients with schizophrenia.
American Journal of Psychiatry, 151, 228-232.
D'Augelli Anthony,
and Hershberger, Scott (1993). Lesbian, gay, and bisexual youth in
community settings: personal challenges and mental health problems. American
Journal of Community Psychology, 21, 421-448.
de Kuyper E (1993).
The Freudian construction of
sexuality: the gay foundations of heterosexuality and straight homophobia.
Journal of Homosexuality, 24(3/4), 137-44.
de Luze, Hubert (1990).
Regards ethnométhodologiques sur le mensonge dans le village des dragueurs
homosexuels parisiens du 15-11-1989 au .15-4-1990. Université de Paris,
Diplôme D'Etude Supérieures Spécialisées. "Title" Internet Page: -
http://www.ai.univ-paris8.fr/corpus/deluze/homemens.htm . "Conclusion"
Internet Page -
http://www.ai.univ-paris8.fr/corpus/deluze/menscon.htm . "Mensonge du
Paraître: Muscles" Internet Page: -
http://www.ai.univ-paris8.fr/corpus/deluze/mens31.htm #muscles .
Dew M, Becker J,
Sanchez J, Caldararo R, Lopez O, Wess J, Dorst S, and Banks G (1997).
Prevalence and predictors of depressive, anxiety and substance use disorders in
HIV infected and uninfected men: a longitudinal evaluation . Psychological
Medicine, 27(2), 395-409.
Dillard-Rosen,
Sandra (1993). Redeeming moment too late to save talk. Denver Post,
August 27, F30. Quoted in Boney(1996).
Doll L, Joy D,
Bartholow B, Harrison J, Bolan G, Douglas J, Saltzman L, Moss P, and Delgado W
(1992). Self-reported childhood and adolescent sexual abuse among adult
homosexual and bisexual men. Child Abuse & Neglect, 16(6), 855-64.
Donaldson,
Stephen (1993). A million Jockers, Punks, and Queens. Internet
Availability: -
http://www.spr.org/docs/prison-sex-lecture.html .
Dorais, Michel
(1994). La recherche des causes de l'homosexualité: une science-fiction?
In Daniel WELZER-LANG, Pierre DUTEY, and Michel Dorais, Eds. La peur de
l'autre en soi, du sexisme à l'homophobie. Montréal: V.L.B.. Internet
Availability:
http://www.europrofem.org/02.info/22contri/2.07.fr/livr_dwl/peur/dwlpeur2.htm
- Table of Contents:
http://www.europrofem.org/02.info/22contri/2.07.fr/livr_dwl/peur/dwlpeur0.htm
Dowsett, Gary
(1994). Working-class homosexuality, gay community, and the masculine
sexual (dis)order. Revue Sexologique, 2(2). Internet Availability: -
http://www.unites.uqam.ca/dsexo/Revue/Vol2no2/2102a5.html .
DuRant R, Krowchuk
D, and Sinal S (1998). Victimization, use of violence, and drug use at
school among male adolescents who engage in same-sex sexual behavior.
Journal of Pediatrics, 133(1), 113-118.
Earls Christopher,
and David, Helene (1989). A psychosocial study of male prostitution.
Archives of Sexual Behavior, 18(5), 401-19.
Ellis, Havelock
(1906). Sexual Inversion. In Havelock Ellis. Studies in
the Psychology of Sex. New York: Random House. Cited edition: Volume 1,
Random House, 1942. First published in 1896 (Wikholm, 1999).
Internet Information: Sexual Inversion: Havelock Ellis' Apology for
Homosexuality Against Victorian Prudishness. -
http://www.albion.edu/student/kstandre/sex.htm .
Englert, Lucianne
(1995). Sexual Orientation. Research & Creative Activity, 27, 2.
Internet Availability: -
http://www.indiana.edu/~rcapub/v18n2/p23.html .
Faulkner, Anne,
and Cranston, Kevin (1998). Correlates of same-sex sexual behavior in a
random sample of Massachusetts high school students. American Journal
of Public Health, 88(2), 262-266. Summary of Massachusetts' 1993 YRBS results: -
http://www.virtualcity.com/youthsuicide/gbsuicide3.htm#24a -
http://www.sws.soton.ac.uk/gay-youth-suicide/2i-youth-risk-behavior-survey.htm#24a
Fergusson D,
Horwood L, and Beautrais A (1999). Is sexual orientation related to
mental health problems and suicidality in young people? Archives of General
Psychiatry, 56(10), 876-880. Internet Availability: -
http://archpsyc.ama-assn.org/issues/v56n10/rfull/yoa9081.html . For
commentaries on research results see Friedman (1999),
Remafedi (1999), and Bailey (1999).
Finkelhor, David
(1979). Sexually Victimized Children. New York: Free Press.
Flavin D, Franklin
J, and Frances R (1986). The acquired immune deficiency syndrome (AIDS)
and suicidal behavior in alcohol-dependent homosexual men. American Journal
of Psychiatry, 143(11), 1440-2.
Forstein Marshall
(1994). Suicidality and HIV in gay men. In: SA Caldwell, RA
Brunham Jr., M Forstein, Eds. Therapists on the frontline:
Psychotherapy with gay men in the age of AIDS. Washington, DC: American
Psychiatric Press, Inc., 111-145.
Foster, Marc (1997).
Nineteen. XY Magazine, 6 , February / March, 20-21.
Foucault, Michel
(1976). La Volonté de savoir. Paris: Gallimard.
Frances RJ,
Wikstrom T, Alcena V (1985).Contracting AIDS as a means of committing
suicide. American Journal of Psychiatry, 142(5), 656 (letter).
Friedman R (1999).
Homosexuality, psychopathology, and suicidality. Archives of General
Psychiatry, 56(10), 887-8. Internet Availability: -
http://archpsyc.ama-assn.org/issues/v56n10/rfull/ycm9268.html .
Garland, Annne, and
Ziegler, Edward (1993). Adolescent Suicide Prevention. American
Psychologist, 48(2), 169-182.
Garofalo, Robert,
Wolf R, Lawrence M, and Wissow S (1999). Sexual orientation and risk of
suicide attempts among a representative sample of youth. Archives of
Pediatric and Adolescent Medicine, 153(5), 487-93.
Garofalo,
Robert, Wolf R, Kessel S, Palfrey J, and DuRant R (1998). The association
between health risk behaviors and sexual orientation among a school-based sample
of adolescents. Pediatrics, 101(5), 895-902.
Gibson, Paul (1989).
Gay and Lesbian Youth Suicide (1989). In: Feinlieb, MR., ed. Vol.
3: Prevention and Intervention in Youth Suicide, Report of the Secretary's
Task Force on Youth Suicide, U.S. Department of Health & Human Services.
Glassner H and
Strauss H (1967). The discovery of grounded theory: strategies for
qualitative research. Chicago: Strauss, Aldine.
Goldflam, Anne,
Chadwick R, and Brown G (1999). Evaluation and Final Report: ‘Here for Life’
Youth Sexuality project. Western
Australian AIDS Council. PDF Document download is available at -
http://www.q-net.net.au/~freedom/professionals.html .
Goldstein,
Richard (1999). The ‘Faggot’ Factor: The chickens came home to roost at
Columbine High. OC Weekly, May 21-27. Internet Availability: -
http://www.ocweekly.com:80/ink/99/37/news-goldstein.shtml
Gottesman,
Irving, and Groome, Carol (1997). HIV/AIDS Risks as a Consequence of
Schizophrenia. Schizophrenia Bulletin, 23(4), 675-684.
Green, Richard
(1987).The "SISSY BOY SYNDROME" and the Development of Homosexuality.
New York: Vail-Ballou Press.
Guide (1999). Gene Scam? The media seized upon a
study suggesting the existence of a 'gay gene.' Now that it is unraveling, mum's
the word. Guide Magazine, January, 1999. Internet:
http://www.guidemag.com/magcontent/invokemagcontent.cfm?ID=C5352D91-2D9E-11D4-A7AD00A0C9D84F02&Method=guidefulldisplay
Halperin, David
(2000). How to do the history of male homosexuality. A Journal of Gay and
Lesbian Studies, 6(1), 87-123. Internet Availability: -
http://muse.jhu.edu/journals/journal_of_lesbian_and_gay_studies/v006/6.1halperin.html
.
Hamer, Dean, Hu S,
Magnuson V, Hu N, and Pattatucci A (1993). A linkage between DNA markers
on the X chromosome and male sexual orientation. Science, 261, 321-327.
Hammelman T (1993).
Gay and lesbian youth: contributing factors to serious attempts or consideration
of suicide. Journal of Gay and Lesbian Psychotherapy. 2(1), 77-89.
Harris, Daniel
(1991). Effeminacy. Michigan Quarterly Review, 30(2).
Harry Joseph (1990).
A probability sample of gay males. Journal of Homosexuality, 19(1), 89-104.
Harry, Joseph (1989).
Parental physical abuse and sexual orientation in males . Archives of Sexual
Behavior, 18(3), 251-61.
Hekma, Gert (1994).
"A female soul in a male body": sexual inversion as gender inversion in
nineteen-century sexology. In Gilbert Herdt. Ed. Third Sex,
Third Gender: Beyond sexual dimorphism in culture and history, 213-39.
New York: Zone Books.
Herdt, Gilbert Ed.
(1994). Third Sex, Third Gender: Beyond sexual dimorphism in culture
and history. New York: Zone Books. Abstract / Table of Contents:
http://www.ifge.org/books/third_sex.htm .
Herek G, Gillis J,
Cogan J, and Glunt E (1997). Hate crime victimization among lesbian, gay,
and bisexual adults: prevalence, psychological correlates, and methodological
issues. Journal of Interpersonal Violence, 12(2), 195-215.
Herrell R, Goldberg
J, True W, Ramakrishnan V, Lyons M, Eisen S, and Tsuang M (1999).
Sexual orientation and suicidality: a co-twin control study in adult men,
Archives of General Psychiatry, 56(10), 867-874. Internet availability: -
http://archpsyc.ama-assn.org/issues/v56n10/rfull/yoa8085.html . For
commentaries on the research results see Friedman (1999),
Remafedi (1999), and Bailey (1999).
Hershberger
Scott, Pilkington N, and D'Augelli A (1997). Predictors of suicide
attempts among gay, lesbian, and bisexual youth. Journal of Adolescent
Research, 12, 477-497.
Hockenberry S,
Billingham R (1987). Sexual orientation and boyhood gender conformity:
development of the Boyhood Gender Conformity Scale. Archives of Sexual
Behavior, 16(6), 475-92. Published erratum: Archives of Sexual Behavior, 1988,
17(3), 287
Holmes W (1997).
Association between a history of child sexual abuse and subsequent,
adolescent psychoactive substance use disorder in a sample in a sample of HIV
seropositive men. Journal of Adolescent Health, 20, 414-9.
HRC: The Human Rights
Campaign (1999). 1998 Exit Polls Show Diverse Picture of Identified
Gay, Lesbian, and Bisexual Electorate. Press Release, February, 16. Internet
Page: -
http://www.hrc.org/newsreleases/1999/990216.asp . "The Voter News Service
exit poll was conducted for ABC, CBS, NBC, CNN, Fox and the Associated Press.
The data was purchased by HRC from Voter News Service."
Hu, Stella, Pattatucci
A, Patterson C, Fulker D, Cherny S, Kruglyak L, and Hamer D (1995).
Linkage between sexual orientation and chromosome Xq28 in males but not in
females. Nature Genetics, 11, 248-256.
Humphreys, Laud
(1975). Tearoom Trade: Impersonal Sex in Public Spaces. Aldine
de Gruyter, New York.
Johnson J, Williams
J, Goetz R, Rabkin J, Remien R, Lipsitz J, and Gorman J (1996).
Personality disorders predict onset of Axis I disorders and impaired functioning
among homosexual men with and at risk for HIV infection . Archives of
General Psychiatry, 53, 350-7.
Johnston, William
I. (1995). Retesting and seroconversion. In: William I. Johnston,
Ed.. HIV-Negative: How the uninfected are affected by AIDS.
New York: Insight Books, Plenum Publishing Corporation, 219-234.
Kalichman S,
Kelly J, Johnson J, and Bulto M (1994). Factors associated with risk for
HIV infection among chronic mentally ill adults. American Journal of
Psychiatry, 151:221-227, 1994.
Katz, Jonathan (1995).
The Invention of Heterosexuality. Dutton, New York. Internet
Information:
http://www.achillesheel.freeuk.com/br22_3.html ,
http://www.indiana.edu/~glbtlib/reviews/r01801.html ,
http://www.informinc.co.uk/LM/LM84/LM84_Books.html .
Kelly B, Raphael B,
Judd F, Perdices M, Kernutt G, Burnett P, Dunne M, and Burrows G (1998).
Suicidal ideation, suicide attempts, and HIV infection. Psychosomatics,
39(5), 405-15.
Keppel, Bobbi, and
Hamilton, Alan (1998). Using the Klein Scale to Teach about Sexual
Orientation. Bisexual Resource Center pamphlet. Internet Availability: -
http://www.biresource.org/klein_graph.html .
Kinsey, Alfred,
Pomeroy W, and Martin E (1948). Sexual Behavior in the Human Male.
Philadelphia: W.B. Saunders.
Kinsman, Gary
(1987). The Regulation of Desire: Sexuality in Canada.
Montréal: Black Rose Books.
Kipke D, O'Connor S,
Palmer R, and MacKensie R (1995). Street Youth in Los Angeles.
Archives of Pediatric and Adolescent Medicine, 149, 513-9.
Kotila l, and
Lonnqvist J (1989). Suicide and violent death among adolescent suicide
attempters. Acta Psychiatrica Scandinavia, 79, 453-9.
Krieger, Nancy, and Sidney, Stephen (1997).
Prevalence and health implications of anti-gay discrimination: a study of black
and white women and men in the Cardia Cohort. International Journal of
Health Services, 27(l), 157-76.
Kruks Gabe. (1991).
Gay and lesbian homeless /street youth: issues and concerns. Journal of
Adolescent Health, 12, 513-8.
Lenderking W,
Wold C, Mayer K, Goldstein R, Losina N, and Seage G (1997). Childhood
sexual abuse among homosexual men: prevalence and association with unsafe sex.
Journal of General Internal Medicine, 12(4), 250-3.
Levine, Lynne, and
Beeler, Linda (1997). Sexual Orientation and Youth Suicide. Paper
presented at Defining the Problem and Meeting The Challenge: Third
Bi-Regional Adolescent Suicide Prevention Conference held in
Breckenridge, Colorado, September, 1997. For the Vermont data, relevant
information is available from Kelly Hale at The Vermont Department of Health
(802) 651-1557, or from Shaun Donahue at The Vermont Department of Education
(802) 748-8640.
Lewinsohn P,
Rohde P, and Seeley J (1993). Psychosocial characteristics of adolescents
with a history of a suicide attempt. Journal of the American Academy of
Child and Adolescent Psychiatry, 32, 60-68.
Lewis G (1988).
The correlation between unsafe sexual behaviors and suicidal probability.
PH.D. Thesis, United States International University, DAI Vol. 49-07B, p. 2863,
139 pages.
Lyketsos G, Sakka
P, and Mailis A (1983). The sexual adjustment of chronic schizophrenics:
A preliminary study. British Journal of Psychiatry, 143, 376-382.
MacMillan H,
Fleming J, Trocme N, Boyle M, Wong M, Racine Y, Beardslee W, and Offord D (1997).
Prevalence of child physical and sexual abuse in the community. JAMA,
278, 131-35.
Mandel Laurie (1996).
Heterosexism, sexual harassment, and adolescent gender Identity: a social and
sexual curriculum in junior high. ED.D. Thesis, Hofstra University, DAI, Vol
57-07A, p. 2775, 180 pages.
Marmor, Judd (1981).
The multiple roots of homosexual behavior. In Judd Marmor, Ed. Homosexual
Behavior: A Modern Reappraisal, pp. 3-22. New York; Basic Books.
Marmor, Judd, Ed.
(1965). Sexual Inversion: The Multiple Roots of Homosexuality.
New York: Basic Books.
Marshall John
(1981). Pansies, perverts, and macho men: Changing perceptions of male
homo sexuality. In Kenneth Plummer, Ed. The Making of the Modern
Homosexual. London: Hutchinson.
Martindale,
Steve, Strathdee S, Hogg R, Cornelisse P, Miller M, Devlin B, Montaner, J.
O'Shaughnessy M, Schechter M (1997). Evidence of Psychologic Distress
in a Cohort of Young Gay/Bisexual Men. Paper presented at the BC AIDS Conference
in Vancouver, October, 1997. Internet Page:
http://cfeweb.hivnet.ubc.ca/vanguard/PAPERS/BCAIDS97Steve.html .
Martin R, Cloninger
C, Guze S, and Clayton P (1985). Mortality in a follow-up of 500
psychiatric patients. Archives of General Psychiatry, 42, 58-66.
Massachusetts' Youth
Risk Behavior Survey (1995). Relevant data and from data made available in
Sexual Orientation and Youth Suicide by Lynne Levine & Linda Beeler. Paper
presented at Defining the Problem and Meeting The Challenge: Third
Bi-Regional Adolescent Suicide Prevention Conference held in
Breckenridge, Colorado, September, 1997. Massachusetts' 1995 Youth Risk
Behavior Survey at -
http://www.doe.mass.edu/lss/yrb95/yrb95ltr.html . Data Related to Sexual
Orientation: -
http://www.doe.mass.edu/lss/yrb95/yrb95111.html#c6 . Summary of research
results -
http://www.virtualcity.com/youthsuicide/gbsuicide3.htm#24 -
http://www.sws.soton.ac.uk/gay-youth-suicide/2i-youth-risk-behavior-survey.htm#24
.
Related published papers - Garofalo et al.,
1998, 1999.
Massachusetts' Youth
Risk Behavior Survey (1997). Table of Contents:
http://www.doe.mass.edu/lss/yrbs97/97yrbstoc.html#TOC - Data Related to
Sexual Orientation:
http://www.doe.mass.edu/lss/yrbs97/97yrbs06.html -
http://www.doe.mass.edu/lss/yrbs97/97yrbs08.html - Summary of research
results:
http://www.sws.soton.ac.uk/gay-youth-suicide/2i-youth-risk-behavior-survey.htm#mass97
-
http://www.virtualcity.com/youthsuicide/gbsuicide3.htm#mass97
Massachusetts' 1999
Youth Risk Behavior Survey should soon become accessible via index Internet
Page at -
http://www.doe.mass.edu/lss/program/youthrisk.html - Table of Contents:
http://www.doe.mass.edu/lss/yrbs99/
Mazza, James (1997).
School-based suicide prevention programs: are they effective? School
Psychology Review, 25(2), 382-98.
McDermott B,
Sautter F, Winstead D, and Quirk T (1994). Diagnosis, health beliefs, and
risk of HIV infection in psychiatric patients. Hospital and Community
Psychiatry, 45, 580-585.
McKirnan D, and
Peterson P (1989). Alcohol and drug use among homosexual men and women:
epidemiology and population characteristics. Addictive Behaviors, 14,
545-53.
Meyer I (1995).
Minority stress and mental health in gay men. Journal of Health and Social
Behavior, 36, 38-56.
Minton, Henry (1995).
Deconstructing Heterosexuality: Life Stories From Gay New York, 1935-1941.
History of Psychology Newsletter, 27(3). Internet Availability: -
http://www.yorku.ca/dept/psych/orgs/apa26/fall95/hetsex.htm
.
Morgan, Fiona (1998).
An audience with the Queen (Interview with Scott Thompson). Salon Magazine, July
23. Internet Page:
http://www.salon.com/ent/int/1998/07/23int.html .
Morgenstern J,
Langenbucher J, Labouvie E, and Miller K (1997). The comorbidity of
alcoholism and personality disorders in a clinical population: prevalence rates
and relation to alcohol typology variables . Journal of Abnormal Psychology,
106(1), 74-84.
Moscicki, Eve
(1995). Epidemiology of suicidal behavior. Suicide and
Life-Threatening Behavior, 25(1), 22-35.
Moscicki Eve
(1989). Epidemiologic surveys as tools for studying suicidal behavior:
A review. Suicide and Life-Threatening Behavior, 19(1), 131-46.
Moscicki, Eve,
Muehrer P, and Potter L (1995). Introduction to supplementary issue:
Research issues in suicide and sexual orientation. Suicide and
Life-Threatening Behavior, 25(Suppl), 1-3.
Morris, Martina,
Zavisca J, and Dean L (1995). Social and sexual networks: their role in
the spread of HIV/AIDS among young gay men. AIDS Prevention and Education,
7(5 Suppl), 24-35.
Moscicki Eve,
O'Carroll P, Rae D, Roy A, Locke B, and Regier D (1989). Suicidal
ideation and attempts; the epidemiologic catchment area study. In:
Report of the Secretary's Task Force in Youth Suicide - Volume 4: Strategies for
the prevention of Youth Suicide edited by Mark L. Rosenburg and Katie
Baer. U.S. Department of Health & Human Services.
Motto J, Heilbron D,
and Juster R (1985). Development of a clinical instrument to estimate
suicide risk . American Journal of Psychiatry, 142(6), 680-6.
Muehrer Peter
(1995). Suicide and sexual orientation: a critical summary of recent
research and directions for future research. Suicide and Life-Threatening
Behavior, 25(suppl), 72-81.
Muehrer, Peter,
Moscicki E, and Potter L (1995). Research issues in suicide and sexual
orientation. Suicide and Life-Threatening Behavior, 25 (Supplement).
Munsey, David (1997).
The Love That Need Not Name its Speaker. National Journal of Sexual
Orientation Law, 2(1). Internet Availability: - Internet:
http://www.ibiblio.org/gaylaw/issue3/munsey.html - Home Page:
http://www.ibiblio.org/gaylaw/
Murphey, Damien
(1998). One in four [young men] face jail sex assault. Sidney
Morning Herald. Internet Availability: -
http://nz.com/NZ/Queer/OUT/news_199806/19980612.html . Related Information:
Joyce C. and O’Hanlon U (1999). There has to be a better way. Law Society
Journal (NSW, Australia). Book Review: David Heilpern, 1998. Fear or favour:
sexual assault of young prisoners. Lismore, Australia: Southern Cross University
Press. Internet:
http://www.lawsocnsw.asn.au/resources/lsj/archive/sep1999/56_3.html .
Murray Stephen, and
Roscoe, Will, Eds. (1998). Boy-Wives and Female Husbands: Studies in
African Homosexualities. New York: St.Martin's Press. Extracts:
http://www.geocities.com/WestHollywood/Stonewall/3044/africa.html -
Blackstripe book review by Reginald Harris:
http://www.blackstripe.com/views/rharris/bwivesfhusb.html - Book Review by
Gert Hekma, University of Amsterdam:
http://www.mask.org.za/sections/ArtsAndCulture/library/review.html
Murray, Stephen et
al. Eds (1992). Oceanic Homosexualities. New York: Garland
Publishing.
Mutchler, Matt
(2000). Seeking Sexual Lives; gay youth and masculinity tensions. In: Peter
Nardi, Ed. Gay Masculinities: Research on Men and Masculinities, pp.
12-43. Thousand Oaks, CA: Sage Publications, Inc..
Newton, Esther
(1993). Cherry Grove, Fire Island: Sixty years in America's first gay
and lesbian town. Boston: Beacon Press.
Nicholas,
Jonathan, and Howard, John (1998). Better dead than gay: depression,
suicide ideation, and attempt among a sample of gay and straight-identified
males aged 18 to 24. Youth Studies Australia, 17(4), 1998, 28-33.
Nilsson, Arne
(1998). Creating their own private and public space in a Nordic city
during high modernity. Journal of Homosexuality, 35(3/4), 81-116.
O'Carroll P, Berman
A, Maris R, Moscicki E, Tanney B, and Silverman M. (1998). Beyond the
tower of Babel: A nomenclature for suicidology. In Kosky et al.,
Eds. Suicide Prevention., 23-39. New York: Plenum Press. Previously
published as O'Carroll P, Berman A, Maris R, Moscicki E, Tanney B, and
Silverman M. (1996). Beyond the tower of Babel: A nomenclature for
suicidology, Suicide and Life-Threatening Behavior, 26(3), 237-52.
Oregon Youth Risk Behavior Survey (1997, 1999).
Results of 1997 survey:
http://www.ohd.hr.state.or.us/chs/teensuic/results.htm . Students were
asked "whether they had been harassed in the previous 30 days and, if so, why.
Two percent of the respondents said they had been because they were perceived to
be gay, lesbian, or bisexual. A related question was asked in 1999, but over a
12-month period. The 1999 survey was to solicit "sexual orientation" information
but someone decided to omit related questions. Results of the 1999 survey:
http://www.sws.soton.ac.uk/gay-youth-suicide/2i-youth-risk-behavior-survey.htm#oregon99
-
http://www.virtualcity.com/youthsuicide/gbsuicide3.htm#oregon99 -
http://www.ohd.hr.state.or.us/chs/yrbs/hs99/yrbs99.htm
Otto U (1972).
Suicidal acts by children and adolescents: A follow-up study. Acta
Psychiatrica Scandinavia, Supplement, 233.
Perkins D, Davidson
E, Leserman J, Liao D, and Evans D (1993). Personality disorders in
patients infected with HIV: a controlled study with implications for clinical
care. American Journal of Psychiatry, 150, 309-15.
Peterson J,
Folkman S, and Bakeman R (1996). Stress, coping, HIV status, psychosocial
resources, and depressive mood in African American gay, bisexual, and
heterosexual men. American Journal of Community Psychology, 24(4), 461-87.
Pharr, Suzanne (1993).
HOMOPHOBIA: A Weapon of Sexism. SIECUS Report, 21(3), 1-4. Internet
Availability: -
http://www.cyfc.umn.edu/Diversity/Gay/siecus.html . The SIECUS article is an
excerpt from Pharr, Suzanne (1998). HOMOPHOBIA: A Weapon of Sexism.
Little Rock, AR: Chardon Press.
Phillips G, and
Over R (1992). Adult sexual orientation in relation to memories of
childhood gender conforming and gender nonconforming behaviors. Archives of
Sexual Behavior, 21(6), 543-58.
Pilkington Neil,
and D'Augelli, Anthony (1995). Victimization of lesbian, gay, and
bisexual youth in community settings. Journal of Community Psychology, 23,
34-57.
Povinelli,
Maryanne, Remafedi G, and Tao G (1996). Trends and predictors of
immunodeficiency virus antibody testing by homosexual and bisexual adolescent
males, 1989-1994. Archives of Pediatric and Adolescent Medicine, 150, 33-38.
Proctor Curtis, and
Groze Victor (1994). Risk factors for suicide among gay, lesbian, and
bisexual youths. Social Work, 39(5), 504-13.
Purkiss, Nathan
(1997). Professionalism, Sexology and Power: Ideology of Homosexuality in
the United States Military. Ex Post Facto, the HSA (History Students
Associations) Journal, San Francisco State University. Internet Availability:
http://www.sfsu.edu/~hsa/ex-post-facto/purkiss.html.
Rado, Sandor (1940).
A critical examination of the concept of bisexuality. Psychosomatic
Medicine, 2, 459-67.
Rahman, Qazi (1999).
Comments on the Neuroanatomy of Human Sexual Orientation and Proposed
Neuroendocrine Hypotheses. Journal of Contemporary Neurology, October. Internet
Availability: -
http://mitpress.mit.edu/e-journals/CONE/articles/004/Rahman.html .
Ramsay, Richard, and
Bagley, Chris (1985). The prevalence of suicidal behaviors, attitudes and
associated social experiences in an urban population. Suicide and
Life-Threatening Behavior, 15(3), 151-67.
Reinherz H,
Giaconia R, Silverman A, Friedman A, Pakiz B, Frost A, and Cohen E (1995).
Early psychosocial risk for adolescent suicidal ideation and attempts.
Journal of the American Academy of Child and Adolescent Psychiatry, 34(5),
599-611.
Reiss, Albert (1961).
The Social Integration of Peers and Queers. Social Problems, 9(2), 197-228.
Reitz, Daniel (1997).
From fisting to Flaubert (Interview with Edmund White). Salon Magazine,
October 15. Internet Page:
http://www.salon.com/books/int/1997/10/15white2.html .
Remafedi, Gary
(1999a). Suicide and sexual orientation: nearing the end of controversy?
Archives of General Psychiatry, 56(10), 885-6. Internet Availability: -
http://archpsyc.ama-assn.org/issues/v56n10/rfull/ycm9279.html .
Remafedi, Gary
(1999). Sexual Orientation and Youth Suicide (Review).
JAMA, 282, 1291-1292. Internet Availability: -
http://www.ama-assn.org/sci-pubs/msjama/articles/vol_282/no_13/jms90031.htm
.
Remafedi, Gary,
Ed. (1994). Death by Denial: studies of suicide in gay and lesbian
teenagers. Alyson Publication, Boston.
Remafedi, Gary
(1994). Predictors of unprotected intercourse among gay and bisexual
youths: knowledge, beliefs, and behavior. Pediatrics, 94(2), 163-168.
Remafedi, G.
(1987). Adolescent homosexuality: psychosocial and medical implications.
Pediatrics, 79(3), 331-7.
Remafedi Gary,
Farrow J, and Deisher R (1991). Risk factors for attempted suicide in gay
and bisexual youth. Pediatrics, 87(6), 869-75.
Remafedi Gary,
French S, Story M, Resnick M, and Blum R (1998). The relationship between
suicide risk and sexual orientation: results of a population-based study.
American Journal of Public Health, 88(1), 57-60.
Rice, George,
Anderson C, Risch N, and Ebers G (1999). Male homosexuality: absence of
linkage to microsatellite markers at Xq28. Science, 284, 665-7.
Rice George, Anderson
C, Risch N, and Ebers G (1995). Male homosexuality: absence of linkage to
micro satellite markers on the X-chromosome in a Canadian study. Poster
presented at the annual meeting of the International Academy of Sex Research.
September 20-24. Provincetown, Massachusetts. Cited by Khytam Dawood, Department
of Psychology, Northwestern University:
http://www.psych.nwu.edu/~khytam/so.html .
Rich, Charles, Fowler
R, Young D, and Blenkush M (1986). San Diego Suicide Study: Comparison of
Gay to Straight Males. Suicide and Life-Threatening Behavior, 16(4), 448-57.
Richardson M,
Myers H, Bing E, and Satz P (1997). Substance use and psychopathology in
African American men at risk for HIV infection. Journal of Community
Psychology, 25(4), 353-70.
Roesler, Thomas,
and Deisher, Robert (1972). Youthful male homosexuality. Journal of
the American Medical Association, 219, 1018-1023.
Rofes, Eric (1995).
Making our schools safe for sissies. In Gerald Unks, Ed.The Gay Teen:
Educational Practice and Theory for Lesbian, Gay, and Bisexual Adolescents,
pp. 79-84. New York: Routledge. Also published in The High School Journal,
77(1/2), 1994, 37-40.
Rofes, Eric (1983).
"I Thought People Like That Killed Themselves:" Lesbians, gay men and suicide.
San Francisco: Grey Fox Press.
Rosenberger P,
Bornstein R, Nasrallah H, Para M, Whitaker C, Fass R, and Rice R (1993).
Psychopathology in human immunodeficiency virus infection: lifetime and
current assessment. Comprehensive Psychiatry, 34, 150-8.
Ross M (1990).
The relationship between life events and mental health in homosexual men.
Journal of Clinical Psychology, 46(4), 402-412 .
Rotheram-Borus, Mary (1993). Suicidal Behavior and risk factors among
runaway youths. American Journal of Psychiatry, 150,103-7.
Rotheram-Borus, Mary, Rosario M, Reid H, and Koopman C (1995). Predicting
patterns of sexual acts among homosexual and bisexual youths. American
Journal of Psychiatry, 152(4), 588-595.
Rotheram-Borus,
Mary, Hunter J, and Rosario M (1994). Suicidal Behavior and Gay-Related
Stress among Gay and Bisexual Male Adolescents. Journal of Adolescent
Research, Vol. 9(4), 498-508. Internet Availability: -
http://www.taasa.org/library/gay_lesbian/gay_lesbian__suicidal.htm .
Saewyc E, Bearinger
L, Heinz P, Blum R, and Resnick M (1998). Gender differences in health
and risk behaviors among bisexual and homosexual adolescents. Journal of
Adolescent Health, 23(3), 181-8.
Sandfort T, Graaf
R, Bijl R, and Schnabel P (1999). Sexual Orientation and Mental Health:
Data from the Netherlands Mental Health Survey and Incidence Study (NEMESIS).
Stony Brook, NY: International Academy of Sex Research. Reference quoted from
Bailey (1999).
San Francisco 1997 Youth
Risk Behavior Survey. Results are available in part 5
of the SSCW (1999) Safe Schools Coalition of WA -
Trainer's Manual at: -
http://www.safeschools-wa.org/ss5train5.html .
Savin-Williams R
(1994). Verbal and physical abuse as stressors in the lives of lesbian,
gay male, and bisexual youths: associations with school problems, running away,
substance abuse, prostitution, and suicide. Journal of Consulting and
Clinical Psychology, 62(2), 261-9.
Scacco, Anthony, Ed.
(1982). Male Rape: A Casebook of Sexual Aggression. New York:
AMS Press.
Schneider
Stephen, Farberow N, and Kruks G (1989). Suicidal behavior in adolescent
and young adult gay men. Suicide Life Threatening Behavior, 19, 381-394.
Schneider,
Stephen, Taylor S, Hammem C, Kemery M, and Dudley J (1991). Factors
influencing suicide intent in gay and bisexual suicide ideators: differing
models for men with and without human immunodeficiency virus. Journal of
Personality and Social Psychology, 61(5), 776-87.
Seal D, Kelly J, Bloom
F, Stevenson L, Coley B, Broyles L (2000). HIV
prevention with young men who have sex with men:
what young men themselves say is needed. AIDS Care, 12(1), 5-26.
Seattle 1Youth Risk
Survey Results (1995). Inormation made available by the Safe Schools
Coalition of Washington (1999). Summaries of Youth Risk
Behavior Survey: Table 4 (p. 10) and Table 6 (p. 15), Eighty-Three Thousand
Youth: Download pdf file:
http://www.safeschools-wa.org/ssc_reports.htm - Home Page:
http://www.safeschools-wa.org/
Sedgwick, Eve
Kosofsky (1993). How to Bring Your Kids Up Gay: The War on Effeminate
Boys. In: Tendencies, pp.154-64. Durham: Duke University Press. A version of
the same essay was also published as "How to bring up your kids gay." In
Michael Warner, Ed. (1993). Fear of a Queer Planet: Queer politics and
Social Theory, pp. 69-81. Minneapolis: University of Minnesota Press.
Sellar C, Hawton K,
and Goldacre, M (1990). Self-poisoning in adolescents; hospital
admissions and death in the Oxford region: 1980-85. British Journal of
Psychiatry, 156, 866-70.
Shaffer David,
Fisher P, Hicks M, and Gould M. (1995). Sexual Orientation in Adolescents
Who Commit Suicide. Suicide and Life-Threatening Behavior, Vol. 25(Suppl.),
64-71.
Shafii M, Carrigan
B, Whittinghill J, and Derick A (1985). Psychosocial autopsy of completed
suicides in children and adolescents. American Journal of Psychiatry, 142,
1061-64.
Siegal, Karolynn;
Meyer, Ilan H. (1999). Hope and resilience in suicide ideation and
behavior of gay and bisexual men following notification of HIV infection.
AIDS Education and Prevention, 11(1), 53-64.
Smith A, Lindsay J,
Rosenthal D (1999). Same-sex attraction, drug injection and binge
drinking among Australian adolescents. Australian and New Zealand Journal of
Public Health, 23(6), 643-6.
SSCW: Safe Schools
Coalition of Washington (1999). The Safe Schools Coalition of WA
Trainers' Manual. Internet Page: -
http://www.safeschools-wa.org/ss5train_index.html . Summaries of School
Survey Results: -
http://www.safeschools-wa.org/ss5train5.html - Index Page:
http://www.safeschools-wa.org/ssc_reports.htm .
Stermac, Lana,
Sheridan P, Davidson A, and Dunn S (1996). Sexual assault of adult males.
Journal of Interpersonal Violence, 11(1), 52-64.
Stiffman A (1989).
Suicide attempts in runaway youths. Suicide and Life-Threatening Behavior,
19(2), 147-59.
Susser E, Valencia
E, Miller M, Tsai W, Meyer-Bahlburg H, Nat R, and Conover S (1995).
Sexual behavior of homeless mentally ill men at risk for HIV. American
Journal of Psychiatry, 152:583-587, 1995.
Telljohann,
Susan, and Price, James (1993). A qualitative examination of adolescent
homosexuals' life experiences: ramifications for secondary school personnel.
Journal of Homosexuality, 26, 41-56.
Tewsbury, Richard
(1996). Cruising for sex in public places: the structure and language of
men's hidden, erotic worlds. Deviant Behavior: An Interdisciplinary Journal,
17, 1-19.
Thorp, John (1992).
The Social Construction of Homosexuality. Phoenix, 46(1), 54-65. Internet
Availability:
http://www.fordham.edu/halsall/med/thorp.html .
Tisdale, Sallie
(1998). Second thoughts. Salon Magazine. September 11. Internet
Availability:
http://www.salon.com/mwt/tisd/1998/09/11tisd.html .
Tompkins-Rosenblatt (1997). Intentional HIV contraction: implications for
direct child and youth care. Residential Treatment for Children and Youth,
14(4), 15-30. Internet Page for abstract:
http://bubl.ac.uk/journals/soc/rtfcay/v14n0497.htm#intentional .
Tremblay Gilles
(1998). Les méandres de l'identité et de l'orientation sexuelle des
hommes. Sexologie Actuelle, janvier. Internet Availability:
http://www.ntic.qc.ca/~blaf/fr/articles/asq_identite.html .
Tremblay, Pierre
(1998-1999). Better to be Dead Than Gay. Internet Page: -
http://www.virtualcity.com/youthsuicide/news/deadly.htm -
http://www.sws.soton.ac.uk/gay-youth-suicide/08-dead-gay-youth-suicide.htm .
A 21-year-old male acted out this ideology via suicide: "A Mother's Letter to
Her Gay Son - Bruce David Ciniello." Internet: -
http://www.virtualcity.com/youthsuicide/news/gay-suicide-mother.htm -
http://www.sws.soton.ac.uk/gay-youth-suicide/08-gay-suicide-mother.htm .
Tremblay, Pierre
(1995). The homosexuality factor in the youth suicide problem. Paper
presented to Sixth Annual Conference of the Canadian Association for Suicide
Prevention, Banff, October, 1995. Internet Availability: -http://www.qrd.org/qrd/www/youth/tremblay/
-
http://www.sws.soton.ac.uk/gay-youth-suicide/tremblay.htm
Tremble, Bob,
Schneider M, and Appathurai C (1989). Growing up gay or lesbian in a
multicultural context. In G. Herdt, Ed. Gay and Lesbian Youth.
New York: Harrington Park Press. Also published in the Journal of Homosexuality,
17(1-4), 1989.
Tuite D, and Luitan J
(1986). 16PF research into addiction meta-analysis and extension. The
International Journal of the Addictions, 21(3), 287-323.
Turner C, Ku L, Rogers S, Lindberg L, Pleck J, and Sonenstein F (1998).
Adolescent sexual behavior, drug use, and violence: Increased reporting with
computer survey technology. Science Magazine, 280(5365-8), 867-73.
Uribe, Virginia, and
Harbeck, Karen (1992). Addressing the needs of lesbian, gay, and bisexual
youth: the origins of PROJECT 10 and school-based intervention. In
Karen Harbeck. Coming out of the Classroom closet: gay and lesbian
students, teachers, and curricula, 9-28. New York; Harrington
Park. Also published in the Journal of homosexuality. 22(3-4), 9-28.
Vermont 1995 (1997,
1999) Youth Risk Behavior Surveys: Relative risk factors for suicide
behaviors of male and female adolescents reporting homo-sex activity compared to
adolescents only reporting hetero-sex activity in 1995 was obtained from a 1997
paper written by Lynne Levine & Linda Beeler which was presented at Defining
the Problem and Meeting The Challenge: Third Bi-Regional Adolescent Suicide
Prevention Conference held in Breckenridge, Colorado. Summary of research
results available at -
http://www.virtualcity.com/youthsuicide/gbsuicide3.htm#25 . Related
published paper: DuRant et al. (1998). Index for the
Vermont 1995, 1997, and 1999 YRBS study results are available at: -
http://www.state.vt.us/adap/ .
Werner Dennis (1998).
Sobre a evolução e variação cultural na homossexualidade masculina. In
Joana Maria Pedro e Miriam Pillar Grossi (orgs).
Masculino, Feminino Plural. Florianópolis: ed. Mulheres, 99-129.
Internet Availability of the English translation "On the
Evolution and Cross-Cultural Variation in Male Homosexuality" by the author):
http://www.iaccess.com.br/~dennis/homosexual.htm .
Weston Kath (1993).
Lesbian/gay studies in the house of anthropology. Annual Review of Anthropology,
22, 339-67.
Wisconsin 1997
Youth Risk Behavior Survey. Results of the question "Have
you ever been threatened or hurt because someone thought you were gay, lesbian,
or bisexual?" are available at: -
http://www.dpi.state.wi.us/dpi/dlsea/sspw/sexual.html .
Voeller, Peter
(1997). Sexual Orientation Lecture Notes. SIGnals Newsletter 4(1)
(Lesbigay Special Interest Group of NAFSA: Association of International
Educators). Internet Page:
http://www.indiana.edu/~overseas/lesbigay/vol4_1/41orientation.htm - SIGnals
Home Page:
http://www.indiana.edu/~overseas/lesbigay/sig.htm
Voice of Connecticut Youth
Survey (1998). Results are available in part 5 of the SSCW (1999)
Safe Schools Coalition of WA - Trainer's Manual at: -
http://www.safeschools-wa.org/ss5train5.html - Voice of Connecticut Youth
Survey Table of Contents:
http://info.med.yale.edu/chldstdy/CTvoices/kidslink/kidslink2/kidsvoice/voice/voicelib/9611-08.html
.
Weinrich, James,
Snyder P, Pillard R, Grant I, Jacobson D, Robinson S, and McCutchan J
(1993). A factor analysis of the Klein sexual orientation grid in two
disparate samples. Archives of Sexual Behavior 22: 157-168. Internet
Availability: -
http://math.ucsd.edu/~weinrich/Kleinfactors.html .
Weldon, Eric (1997).
The trouble with sex. XY Magazine, 6, February / March, 53.
Wikholm, Andrew
(1999). 1896: Ellis Publishes Sexual Inversion. Internet Page: -
http://www.gayhistory.com/rev2/factfiles/ff1896b.htm .
Williams J, Rabkin
J, Remien R, Gorman J, and Ehrhardt A (1991). Multidisciplinary baseline
assessment of homosexual men with and without immunodeficiency virus infection.
II Standardized clinical assessment of current and lifetime psychopathology.
Archives of General Psychiatry, 48, 124-30.
Working Groups
workshop on suicide and sexual orientation (1995). Recommendations for a
research Agenda in Suicide and sexual orientation. Suicide and Life
Threatening Behavior, 25 (Suppl.), 82-88.
Yoshino, Kenji
(2000). The epistemic contract of bisexual erasure. Stanford Law
Review, 53(2), 353-461.